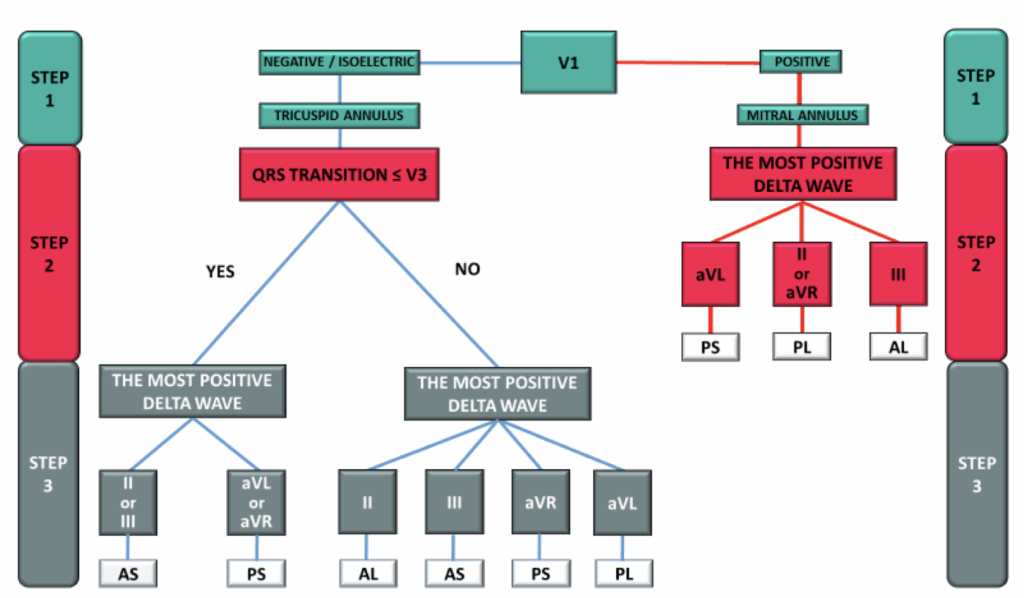
Positive : left sided AP (Mitral annulus), where is the most positive Delta wave
AVL -> post-sep
II/AVR -> post-lat
III -> ant-lat
Negative : right sided AP (Tricuspid annulus), where is the QRS transition
<V3 where is the most positive Delta wave
II / III -> ant-sep
AVL / AVR -> post-sep
>V3 where is the most positive Delta wave
II -> ant-lat
III -> ant-sep
AVR -> post-sep
AVL -> post-lat
El Hamriti M, Braun M, Molatta S, et al. EASY-WPW: a novel ECG-algorithm for easy and reliable localization of manifest accessory pathways in children and adults. Europace. 2022 Dec 12;25(2):600–609. doi: 10.1093/europace/euac216.
Step 2 : Is there a criteria for AP ?
Is there an anterograde AP ? (especially if HV < 35 ms)
Left sided anterograde AP suspected -> pace CS1-2
Right sided anterograde AP suspected -> pace R
Is there a retrograde AP ? -> Test VA conduction
Where is the first activation ?
Is it decremental ?
– First activation : CS1,2 + non decremental -> Left sided AP suspected – First activation : RA + non decremental -> Right sided AP suspected – First activation : CS9,10 + non decremental -> Septal AP suspected – First activation CS9,10 + decremental = Normal
ParaHisien pacing
No modification of the HA -> AP highly suspected
Shortening of the HA with high output -> normal response
Step 3 : Is there a criteria for dual AV node ?
Is there an AH jump ? (> 50 ms AH increase with 10 ms decremental in A1-A2) ?
AVNRT probable
AH jump + Is it associated with an echo beat ?
AVNRT highly probable
AH jump + Echo beat + Is it associated with entrainement of SVT ?
Definite diagnose of AVNRT
Step 4 : Inductie & Observe SVT
Is there a 1:1 relationship between A and V
Yes : it can be AVNRT, AVRT or AT
Missing V : AVRT is unlikely
Missing A : AVRT & AT are unlikely
VA time < 61-70 ms ?
Exclude AVRT
Where is the earliest activation ?
CS1-2 -> AT or AVRT likely
RA -> AT or AVRT likely
CS9,10 / His -> don’t help
Spontaneous termination
End with an A (VAV) -> AVRT or AVNRT likely
End with a V (VAAV) -> AT likely
Is there a variation of AA interval ?
HH interval predict AA interval -> AVNRT / AVRT likely
AA interval predicat HH interval -> AT likely
Step 5 : Ventricular pacing manoeuvres
Ventricular over pacing
VAV response : DEFINITE AVRT or AVNRT 100%
VAAV response : DEFINITE AT 100%
Ventricular overdrive Post-Pacing interval to differentiate between AVRT and AVNRT : PPI-CL
> 115 ms -> AVNRT likely
< 115ms -> AVRT likely
PVC the same time of just before the His (refractory period)