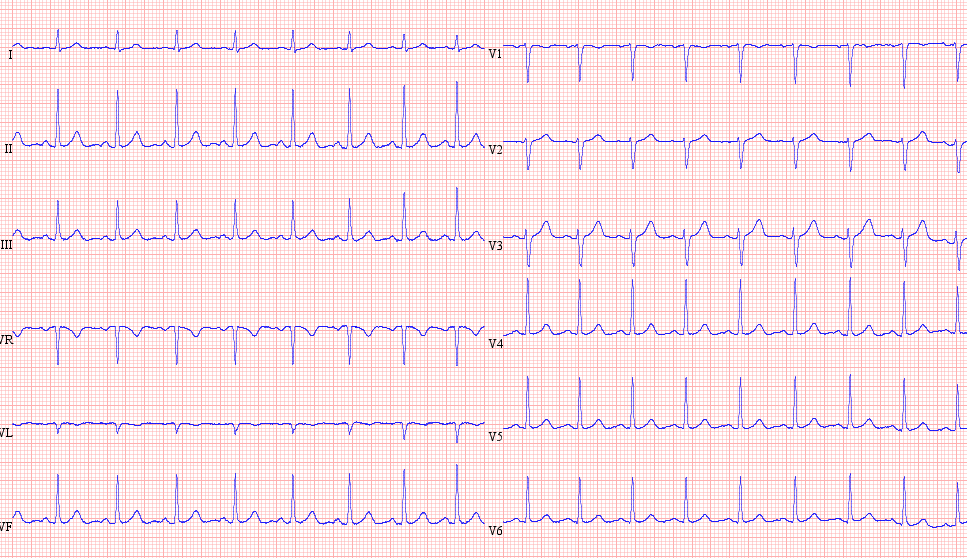
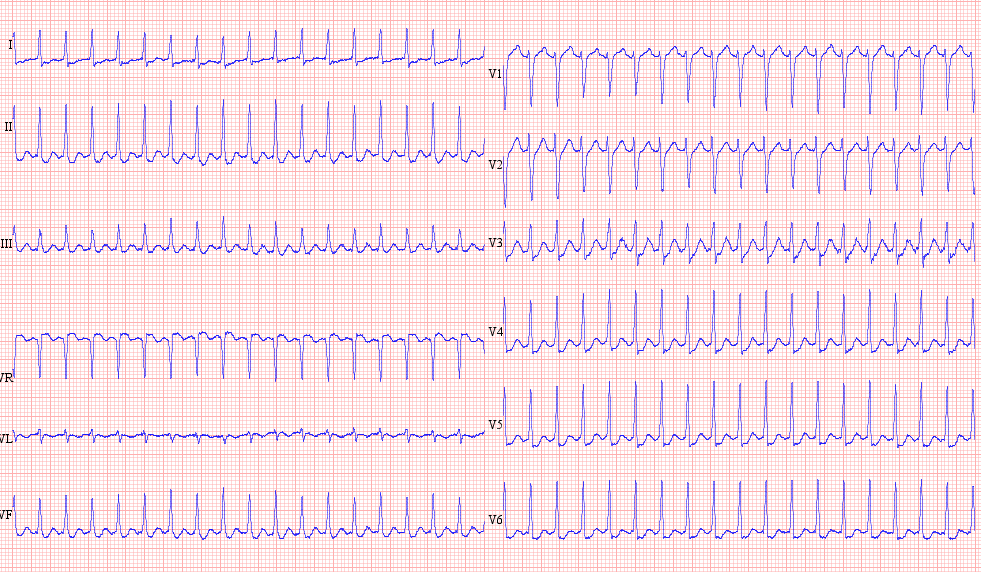
SVT 220 bpm, difficult to say where is the P wave…
It Stops with adenosine
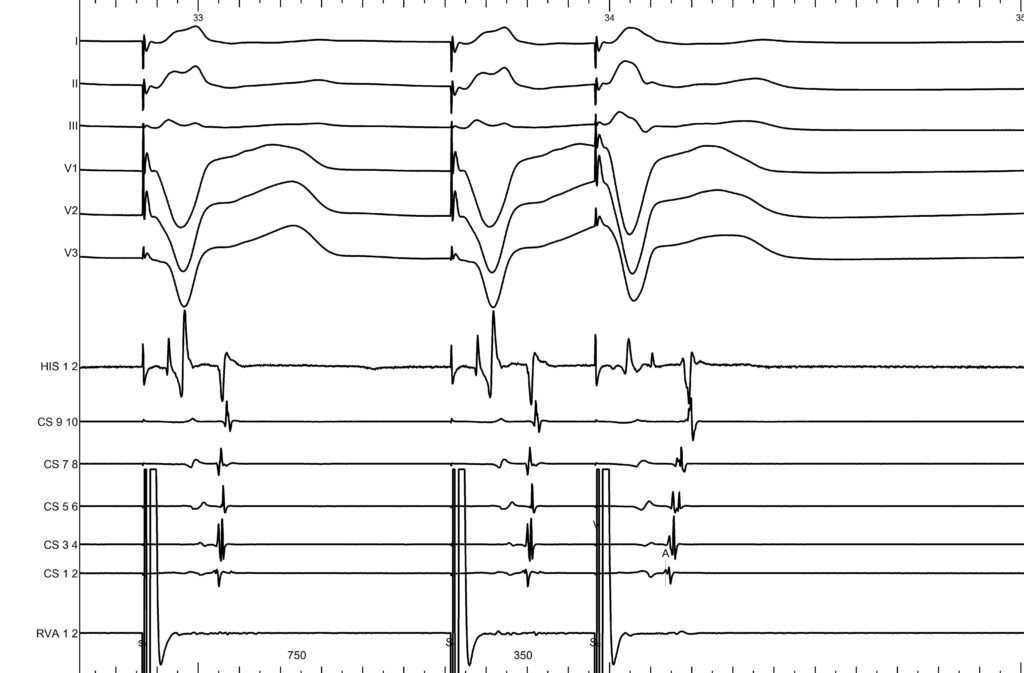
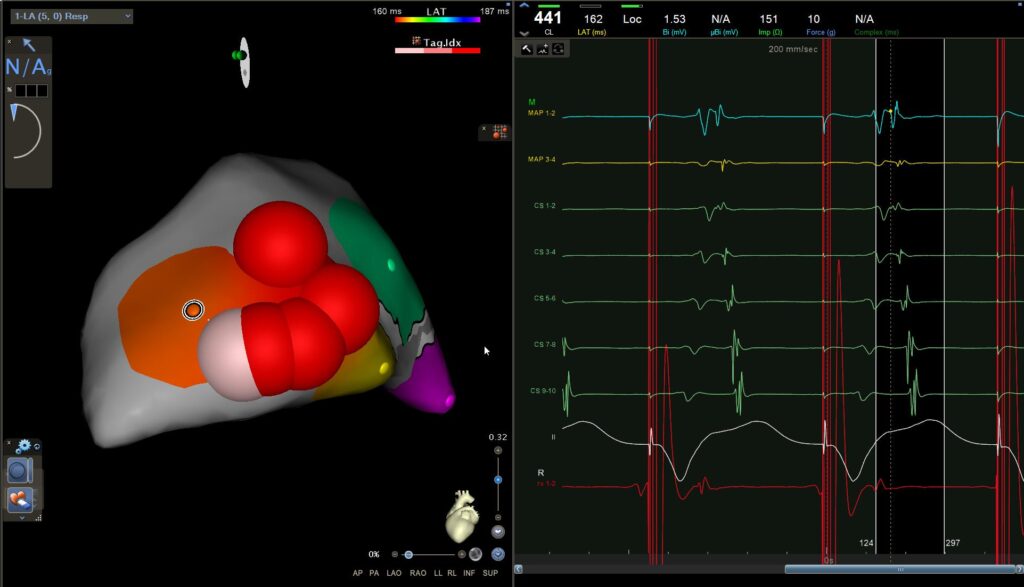
EP study showing a non-decremental, eccentric VA with earliest activation from CS1–2
We move toward the left side, and during ventricular pacing we look for VA fusion — which I see as a kind of ‘pyramidal’ pattern we need to identify. If we examine the signals carefully, the ventricular activation from CS9–10 travels upward and to the right toward the ablation catheter, while the atrial signal from CS9–10 travels upward and to the left. Both wavefronts converge toward the ablation catheter, where they fuse.
You can clearly see on the mapping, at the level of the ablation catheter, that there is a fusion between the atrial and ventricular signals.
We can see that the best localisation is in the posterolateral region.
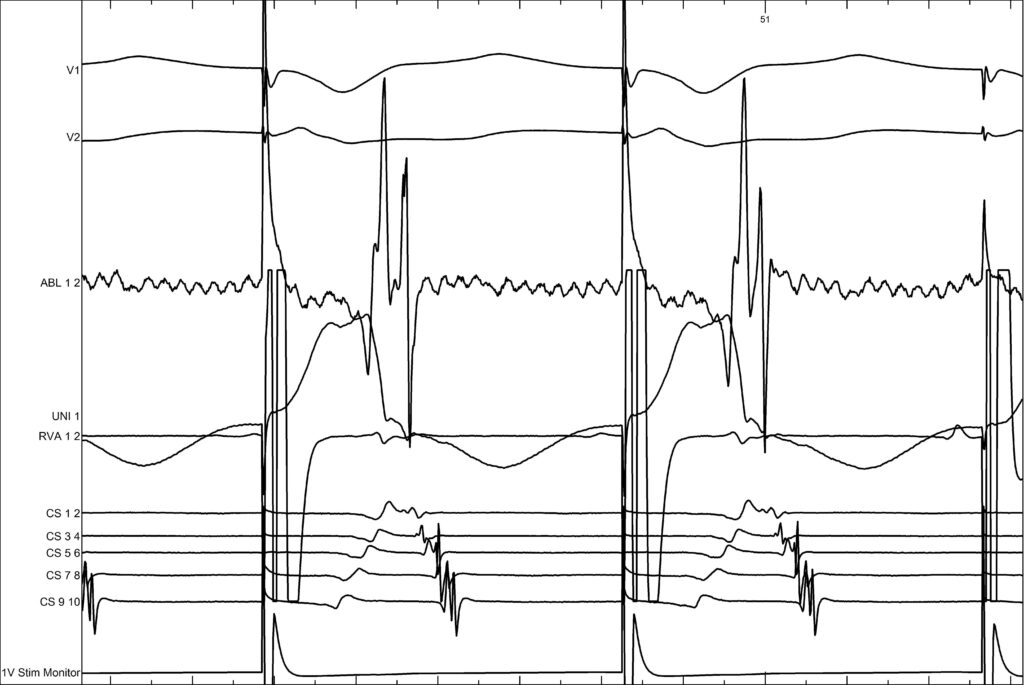
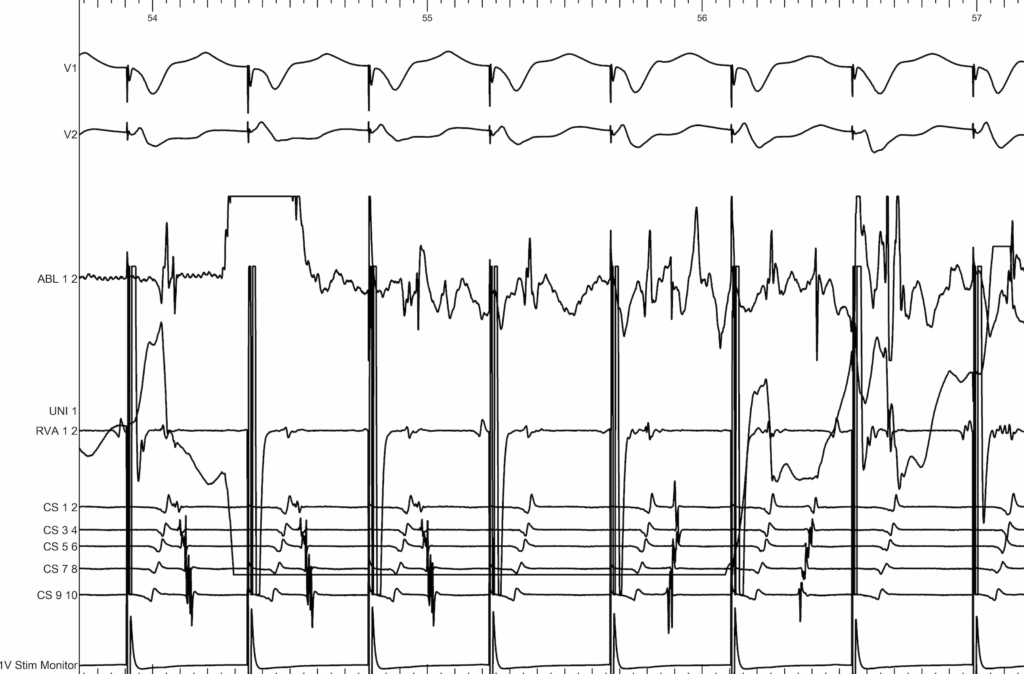
Here we are pacing at the ventricular level. We first see the activation of the CS progressing from CS1,2 toward CS9,10, and immediately after the application there is a change in activation, which becomes normal again, from CS9,10 toward CS1,2.
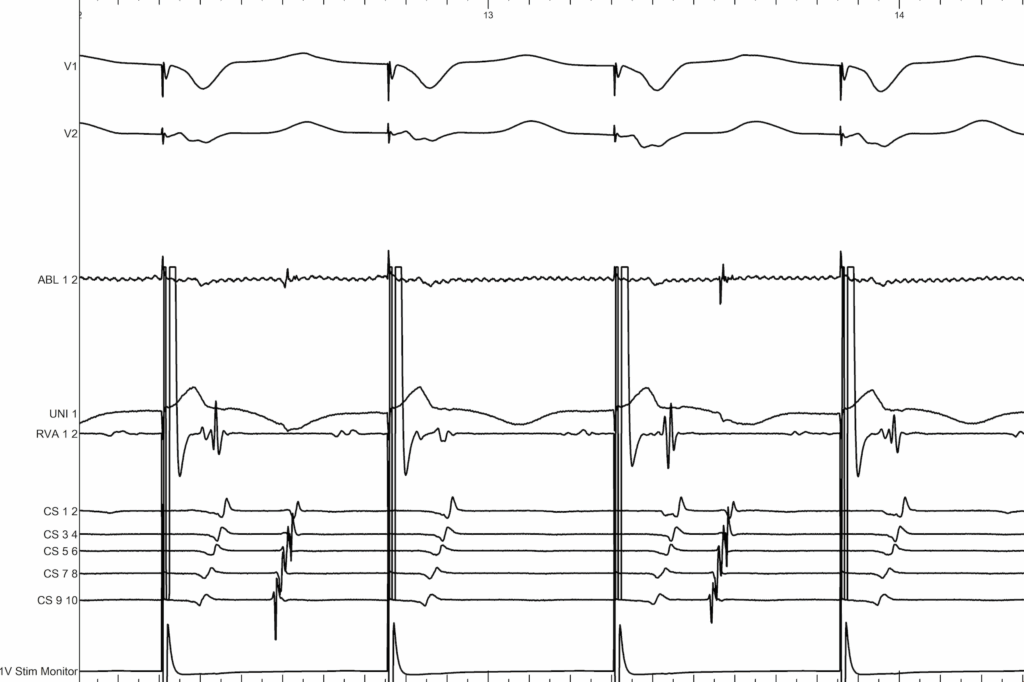
Now we inject adenosine to see whether there is any conduction through the accessory pathway. You can clearly see that after the adenosine injection, the activation remains concentric with block, which confirms that there is no longer any conduction through the accessory pathway