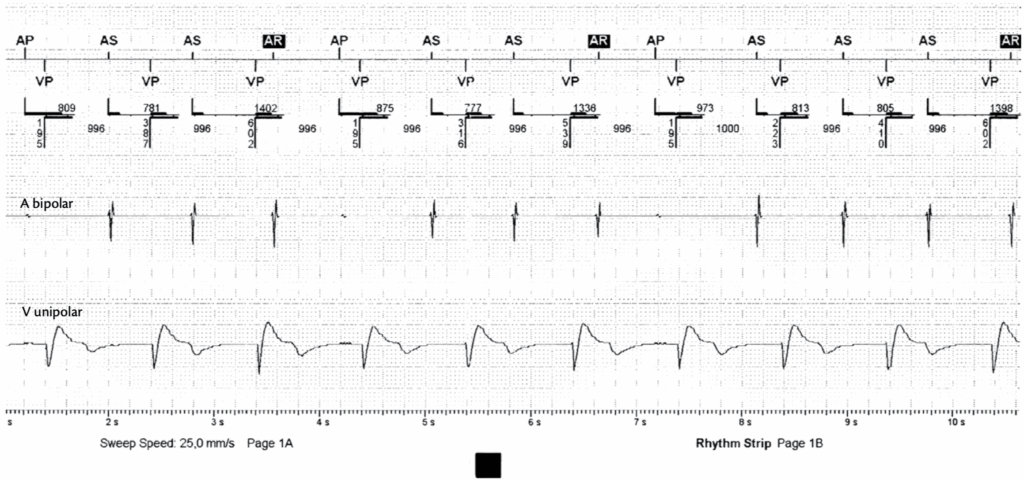
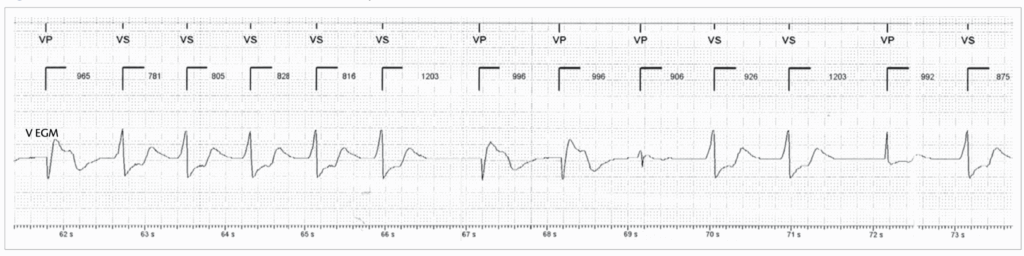
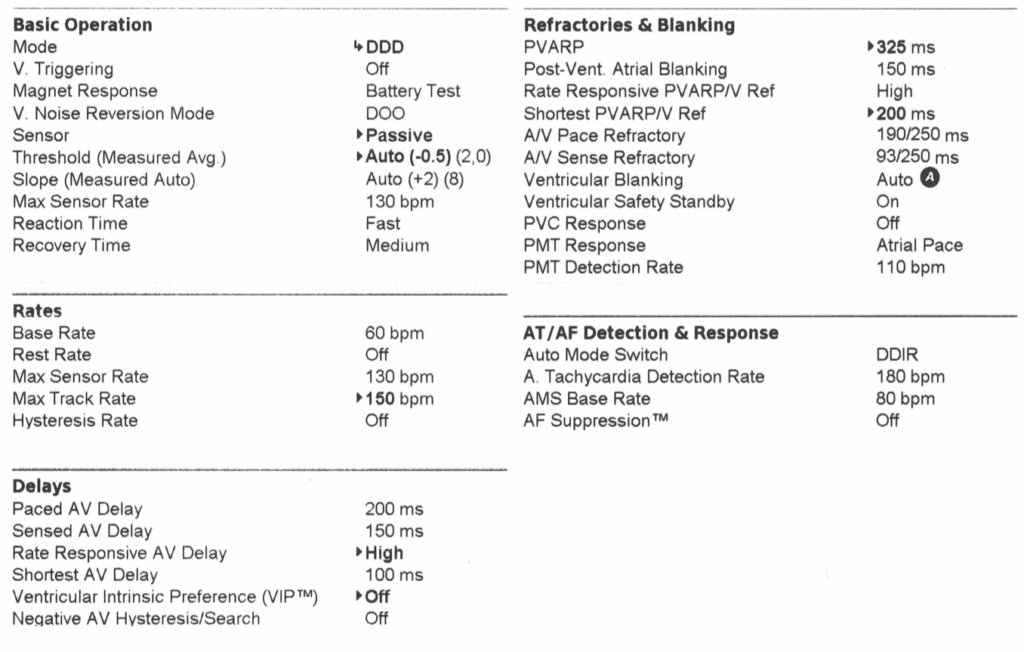
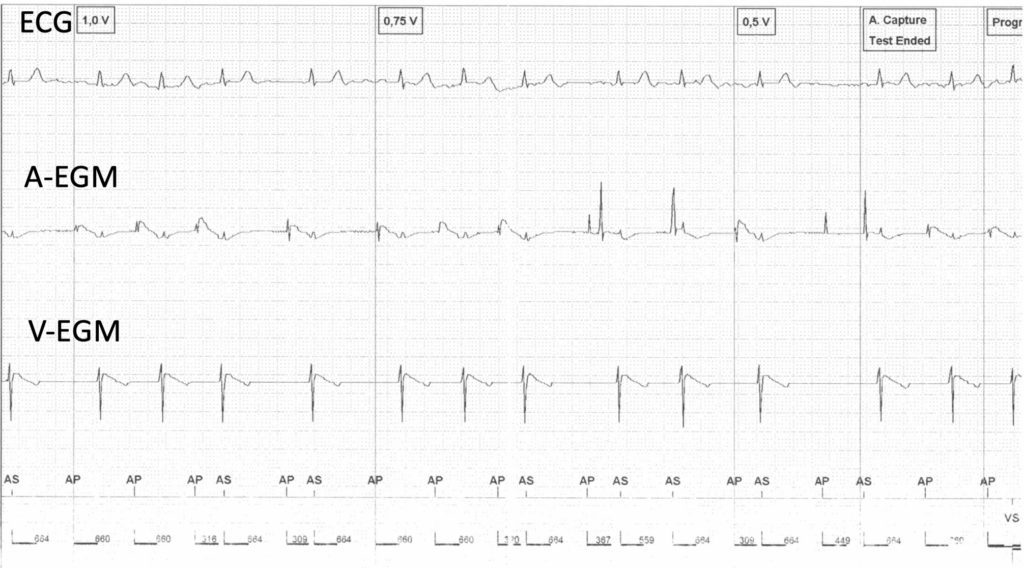
DDI
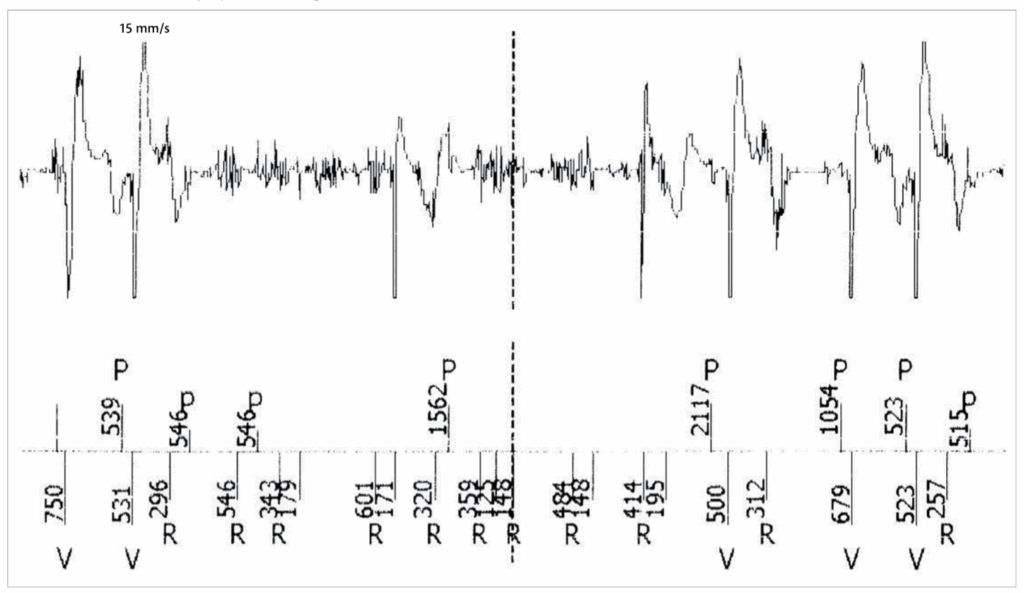
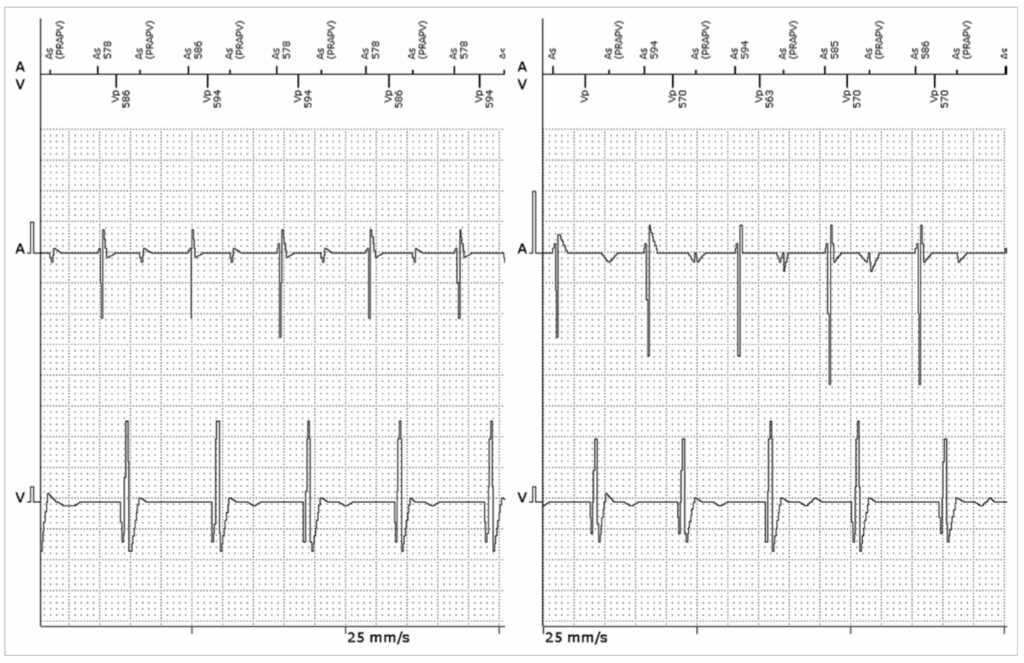
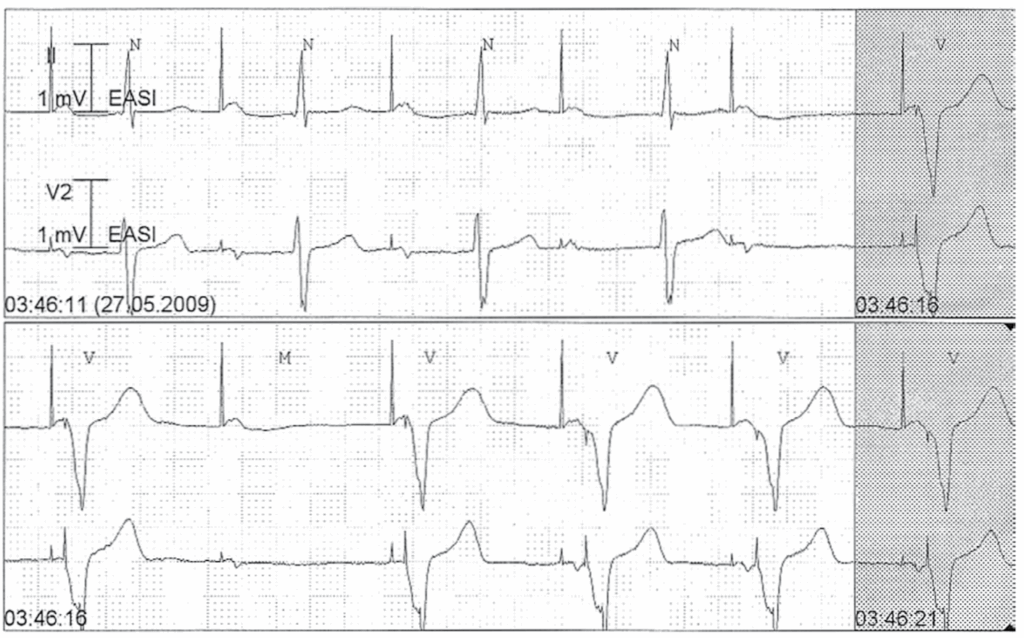
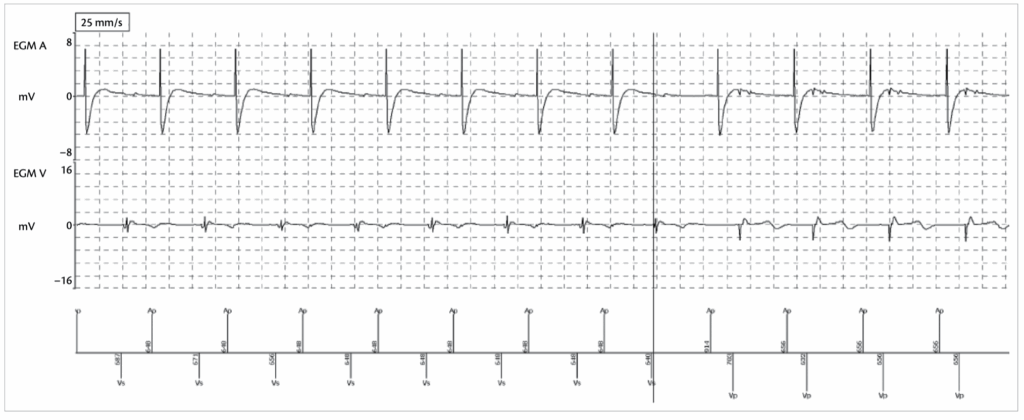
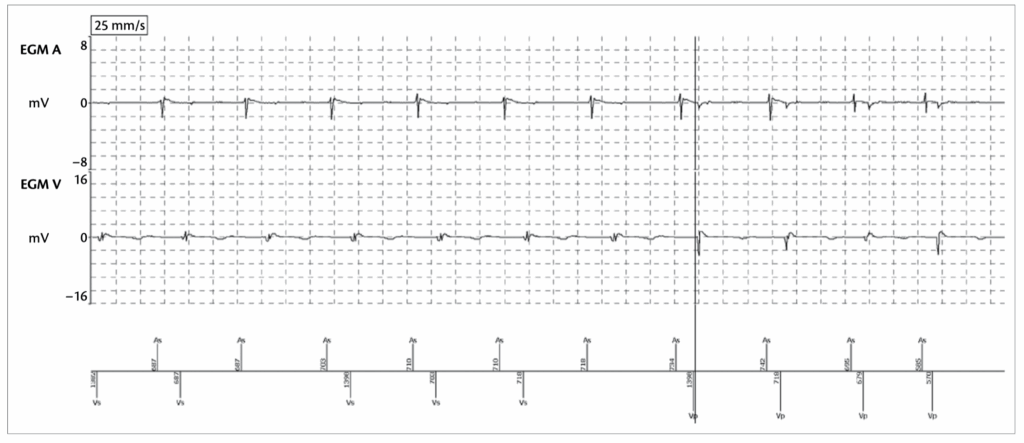
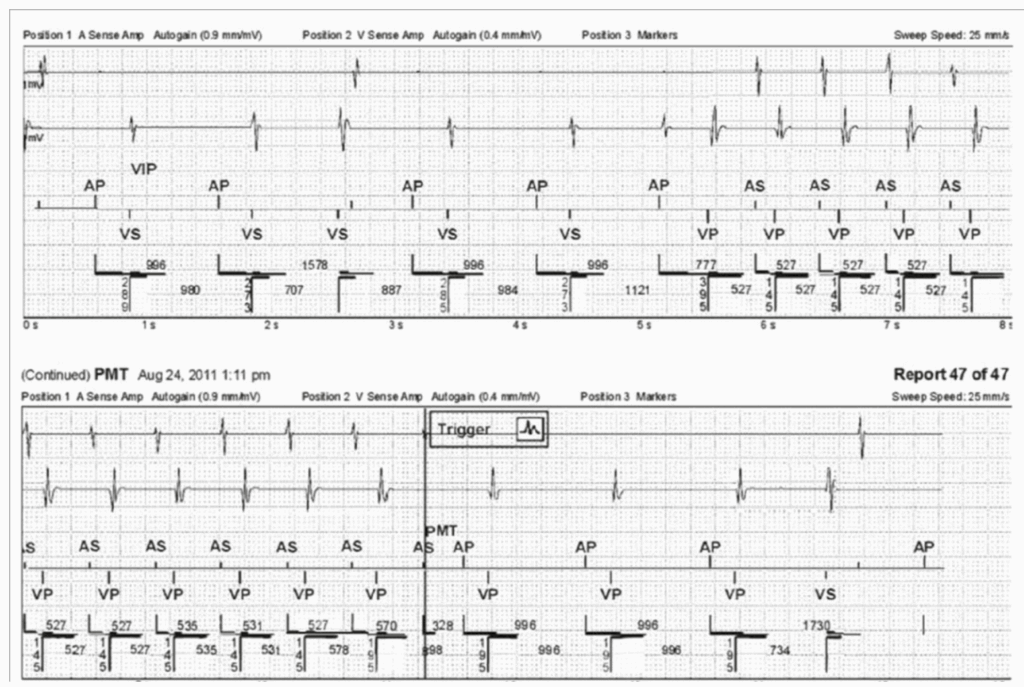
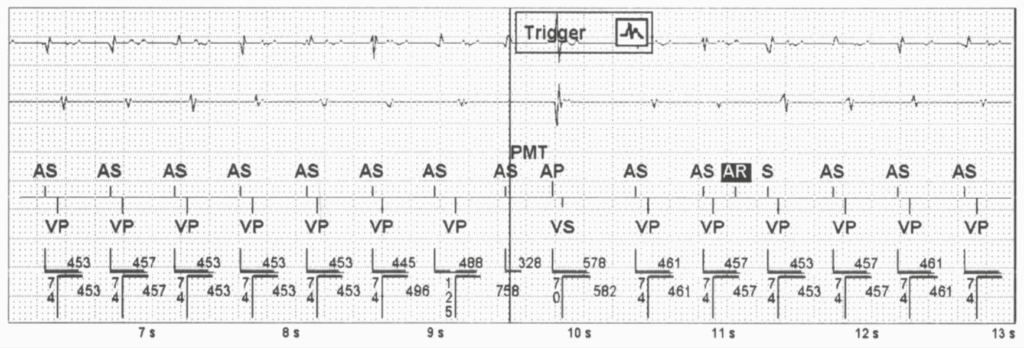
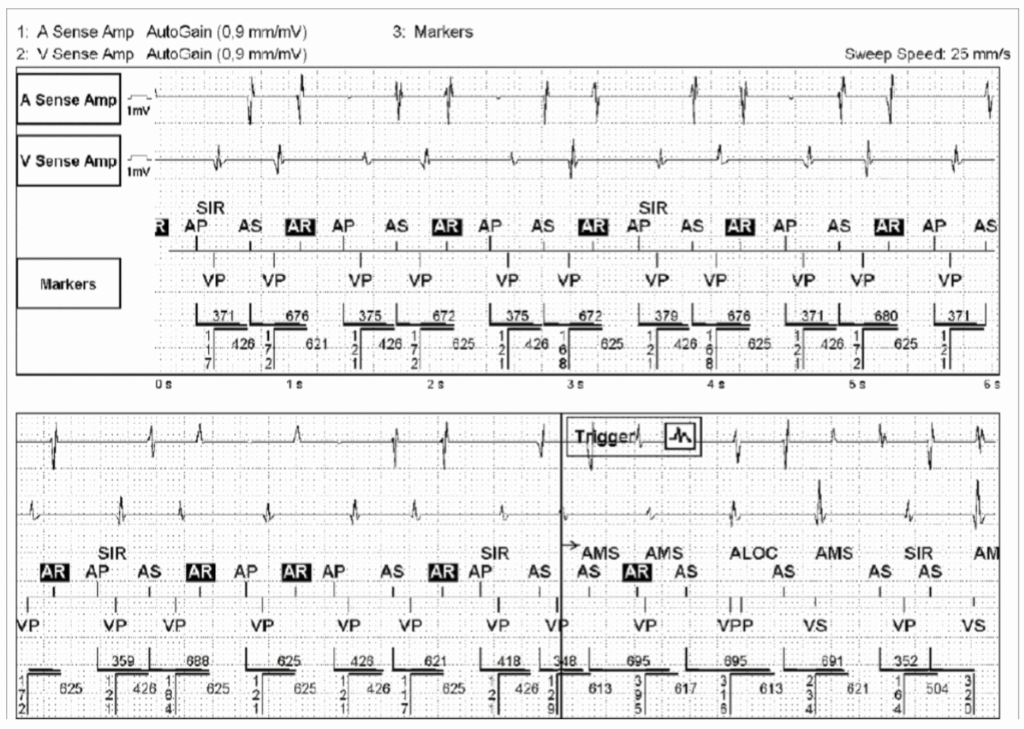
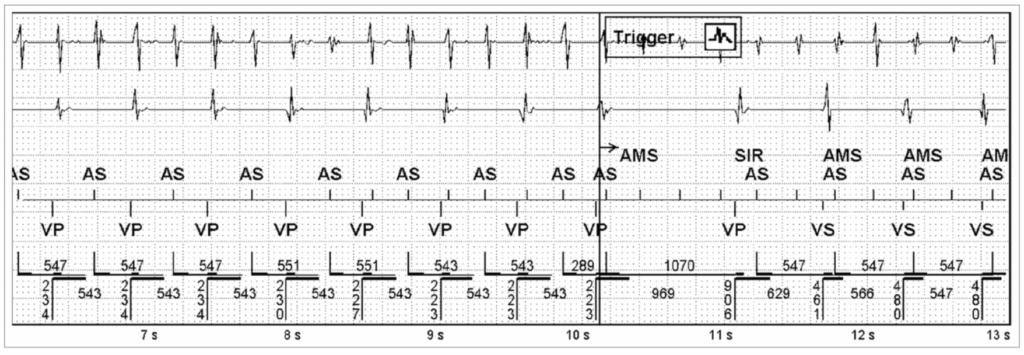
1 – There is loss of AV synchrony with atrial sensed events (AS) at a constant ventricular pacing (VP) rate 60 bpm (VP-VP 996 – 1000 ms) -> this excludes DDD and VDD.
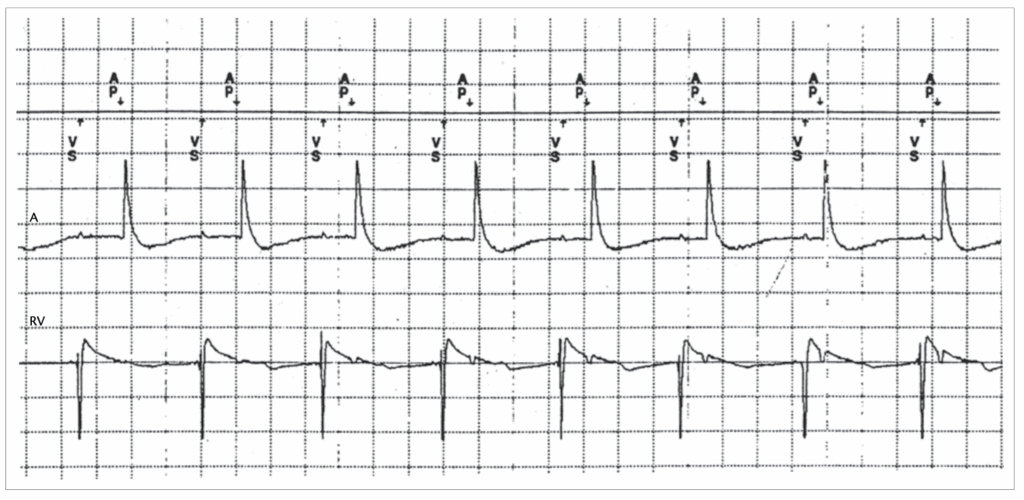
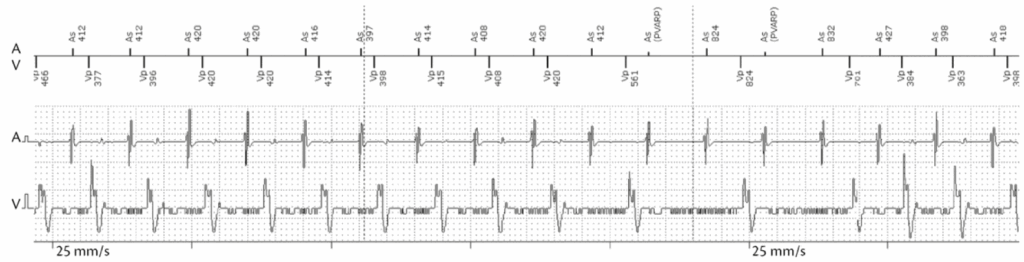
2 – In DDI mode -> VA interval is triggered after a VP or VS events. AR that fall within the PVARP do not inhibit AP.
3 – AP occurs at the end of the VA interval (800 ms).
4 – AV synchrony is maintained after AP events.
Pros :
– To avoid to programme very long AV delays in the DDD mode, to avoid RV pacing
– Atrial tachy-arrhythmias, to avoid rapid ventricular pacing
Cons :
– Asynchrony