 Here’s what we’re seeing in this tracing:
Here’s what we’re seeing in this tracing:
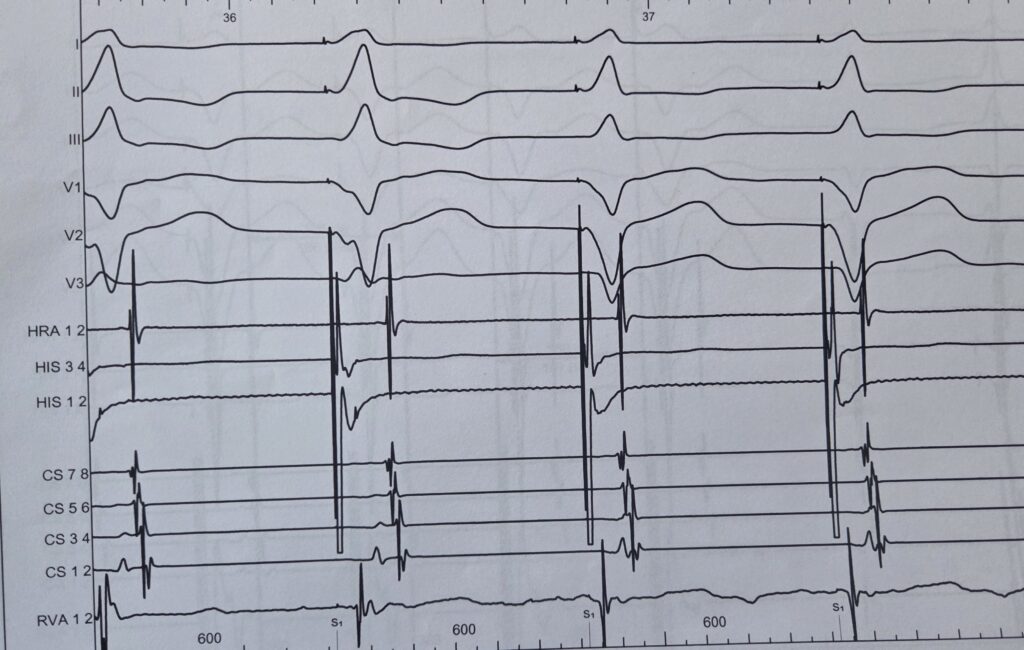
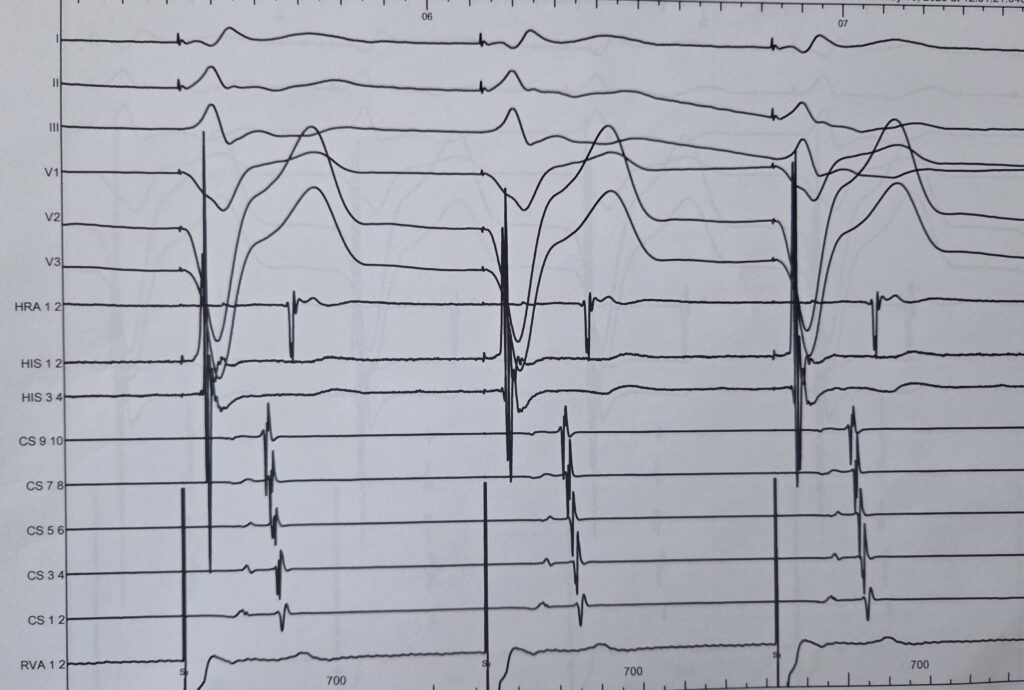
Ventricular pacing check:
We stimulated at 700 ms ⚡️ and observed that activation was concentric for the first and second paced QRS complexes ✅. However, for the third paced QRS, activation within the coronary sinus became eccentric 🔄, starting from CS 5-6 📍.
-> It suggest an accessory pathway
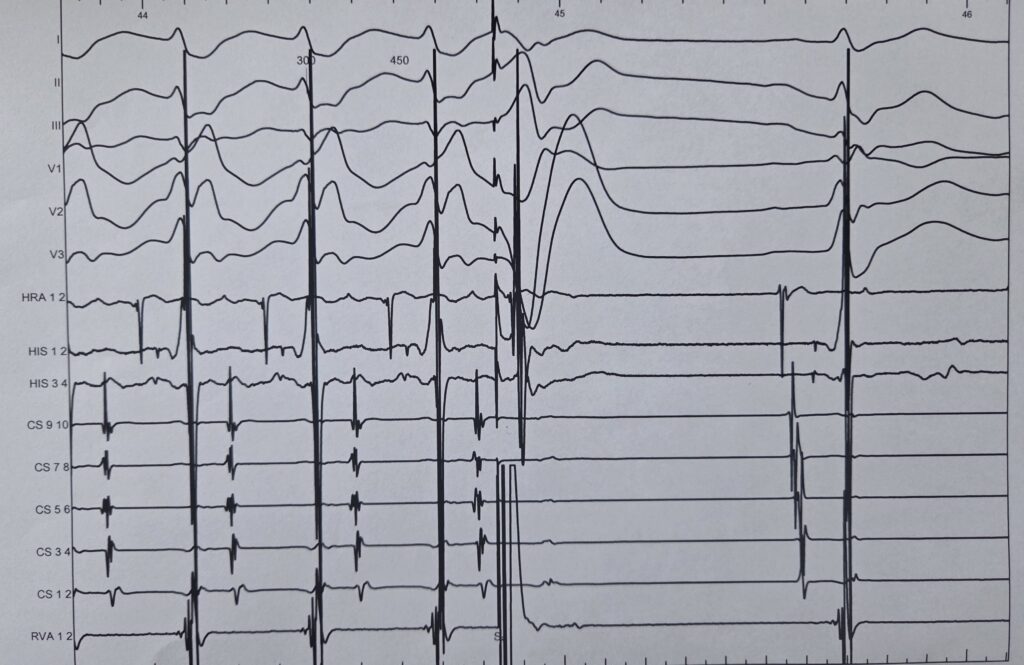
Here’s what we’re seeing in this tracing:
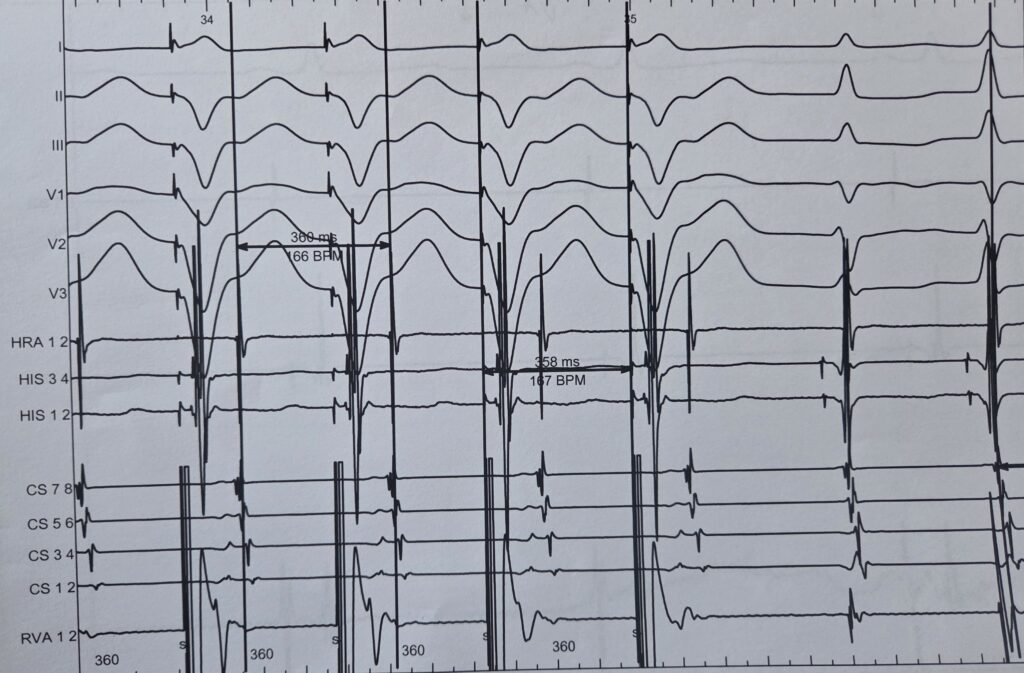
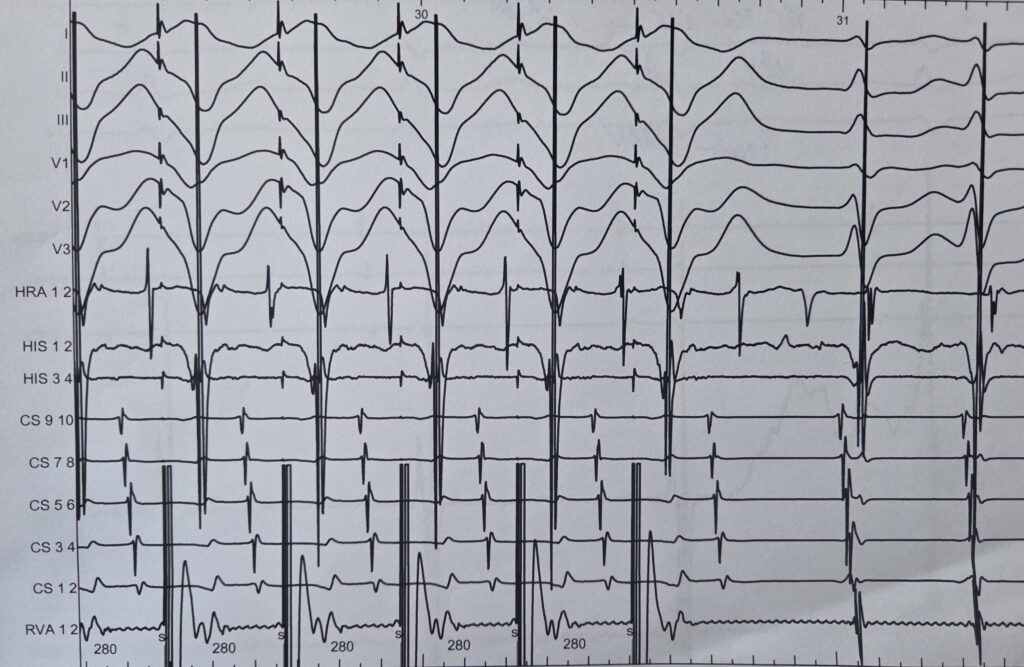
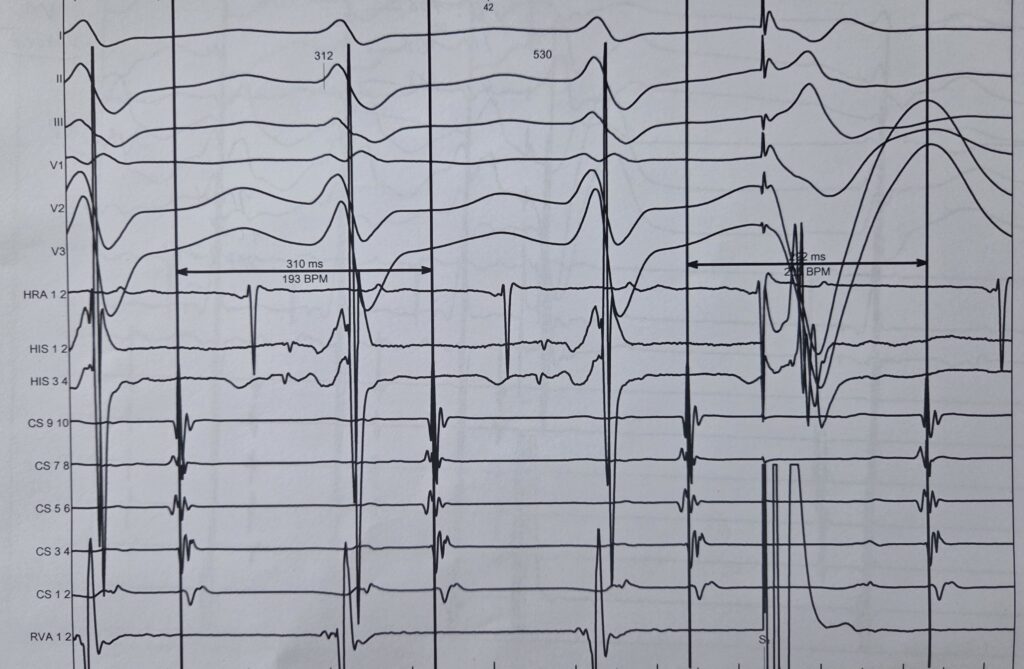
 Tachycardia analysis:
Tachycardia analysis:
Look closely at the last two QRS complexes—the RP interval is not short, strongly suggesting AVRT, atypical AVNRT or AT. 
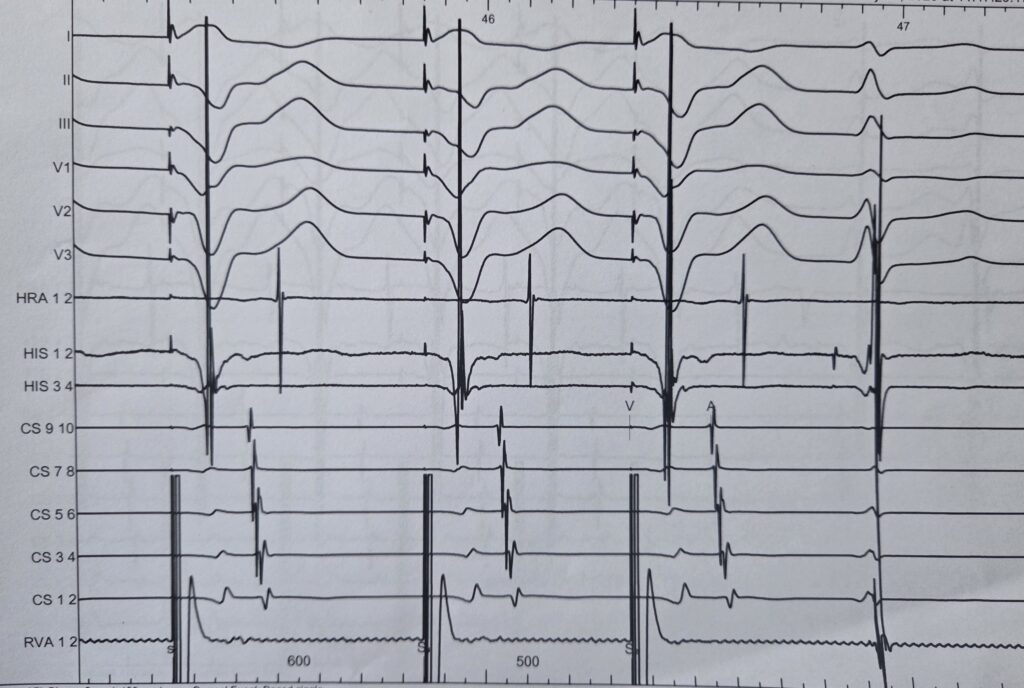
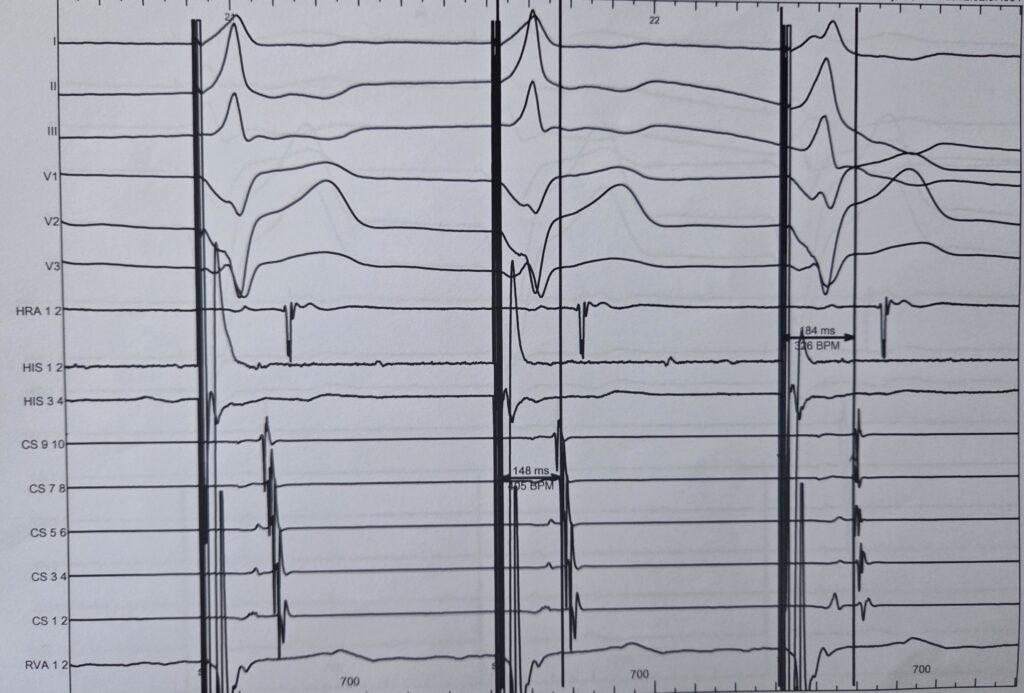
 Extra-Ventricular pacing:
Extra-Ventricular pacing:
Therefore, we paced in the ventricle ⚡️ with an extrastimulus delivered within the refractory period of the His bundle ⏳, resulting in atrial advancement from 310 ms to 290 ms ⬅️.