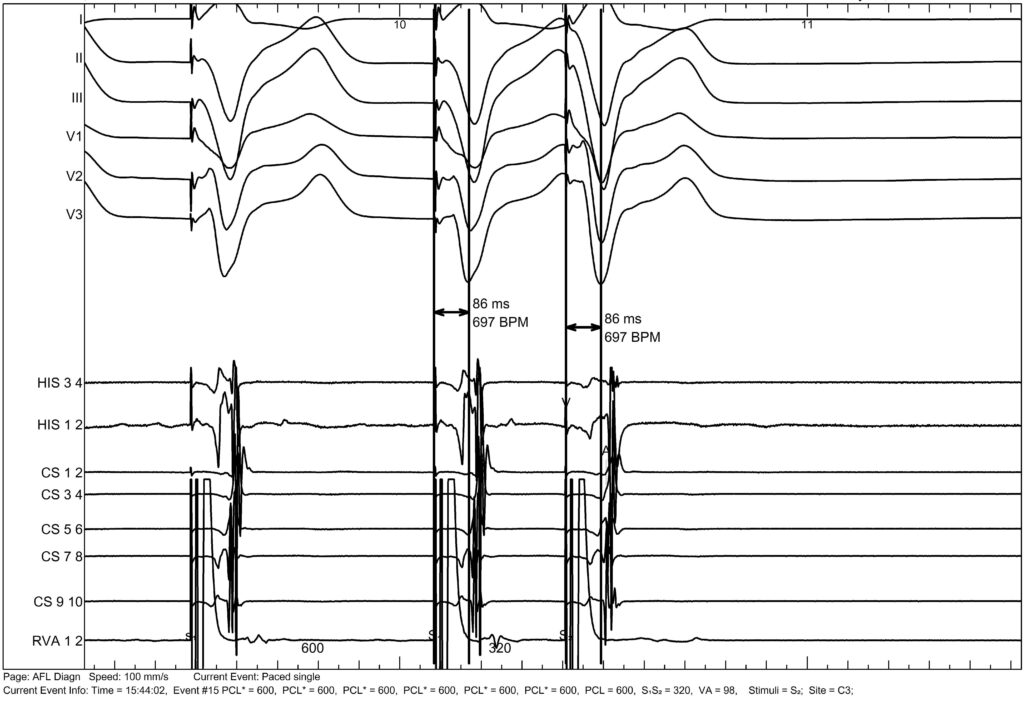
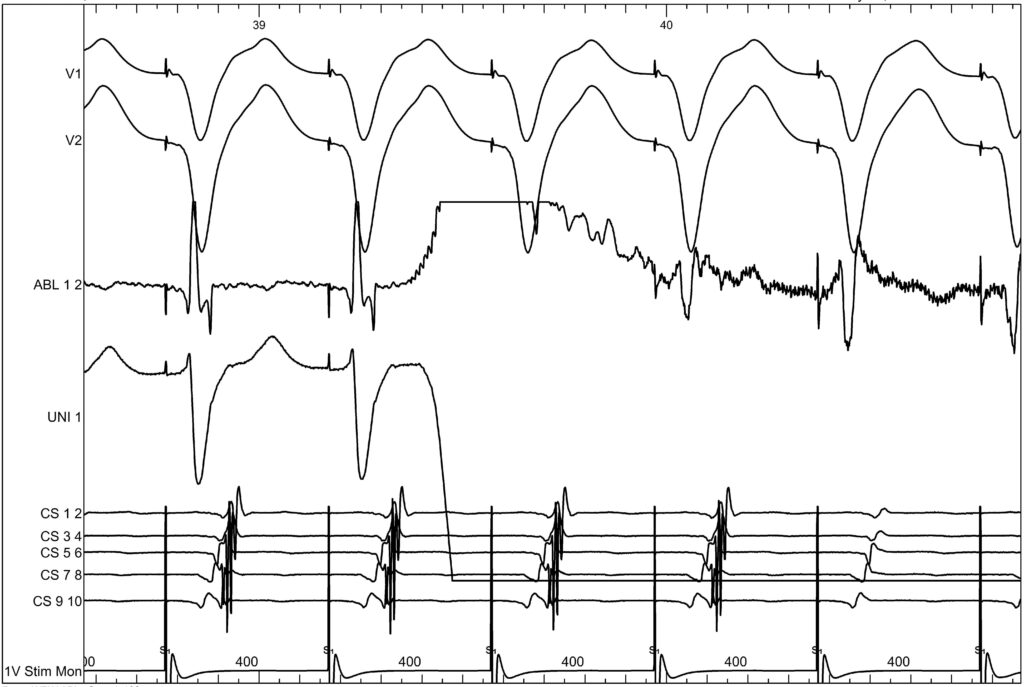
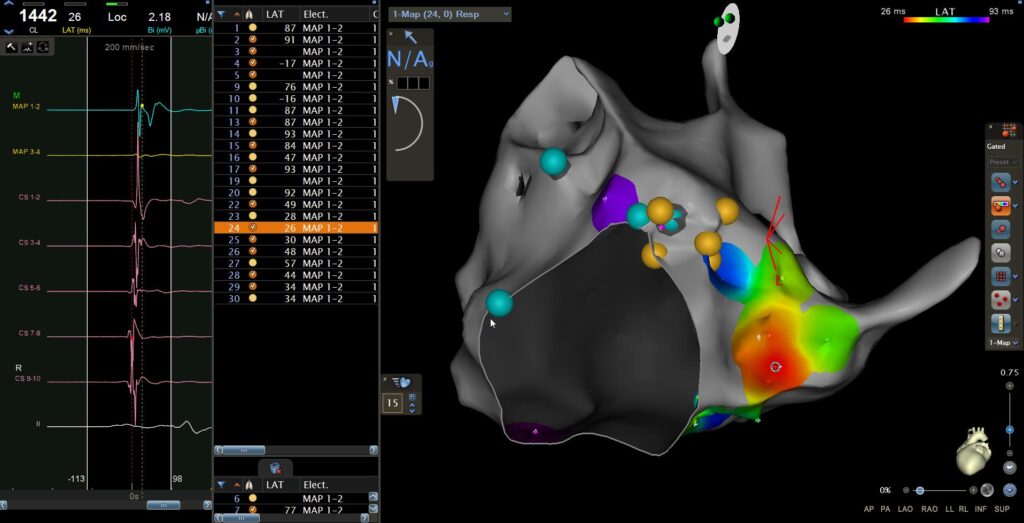
To ablate this concealed accessory pathway, ventricular pacing was performed. The His bundle was first identified, after which VA fusion was sought. Ablation was delivered at the posteroseptal region, resulting in disappearance of accessory pathway conduction within the first three seconds of energy delivery.