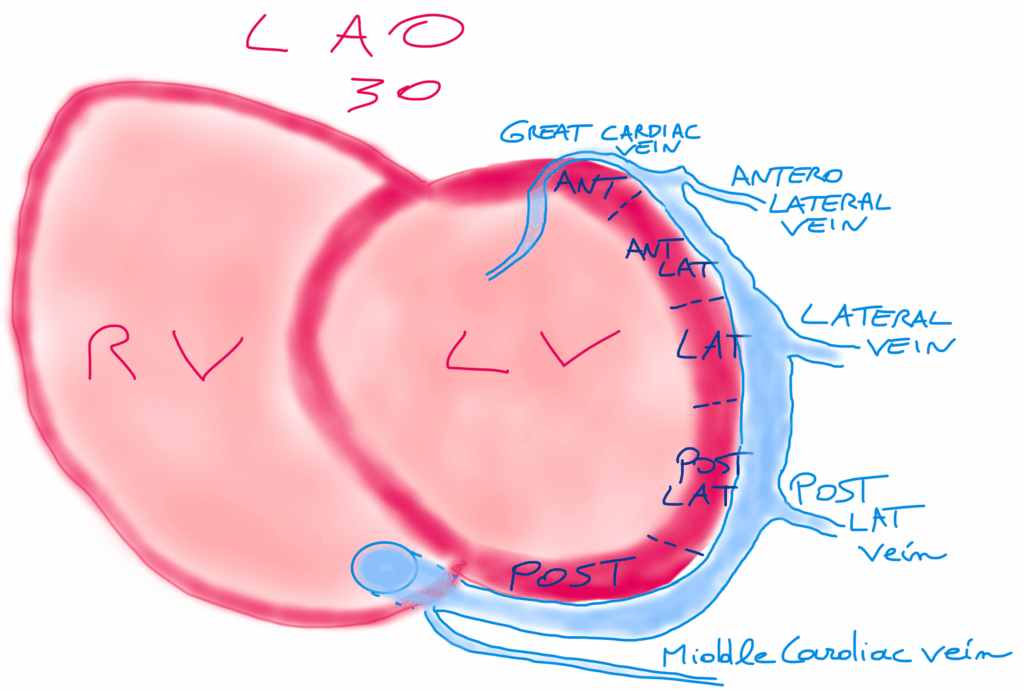
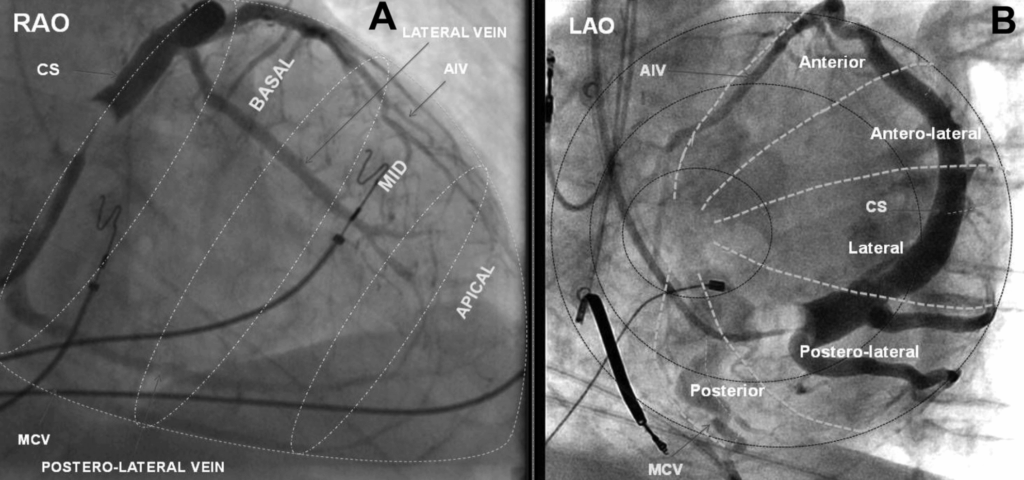
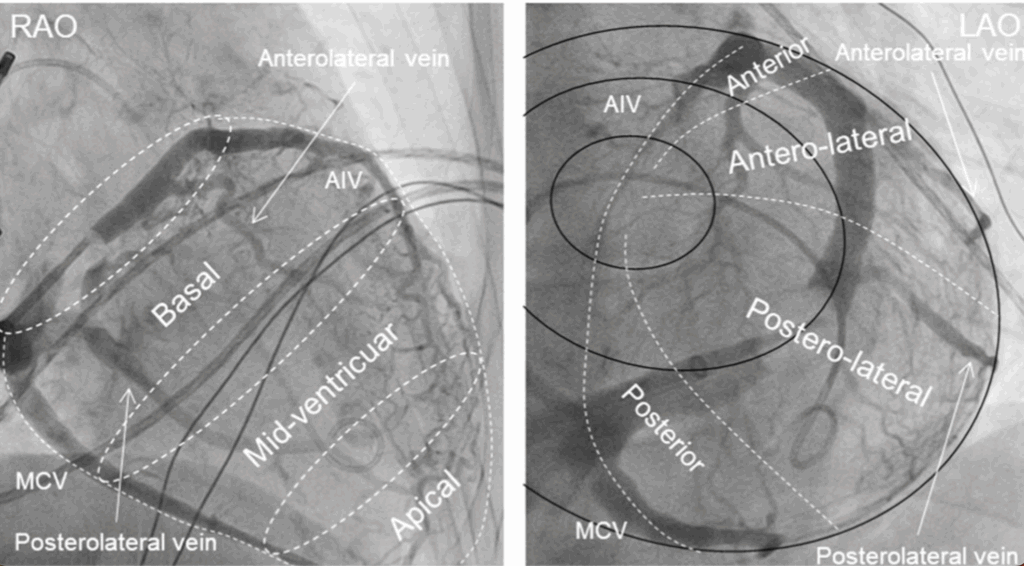
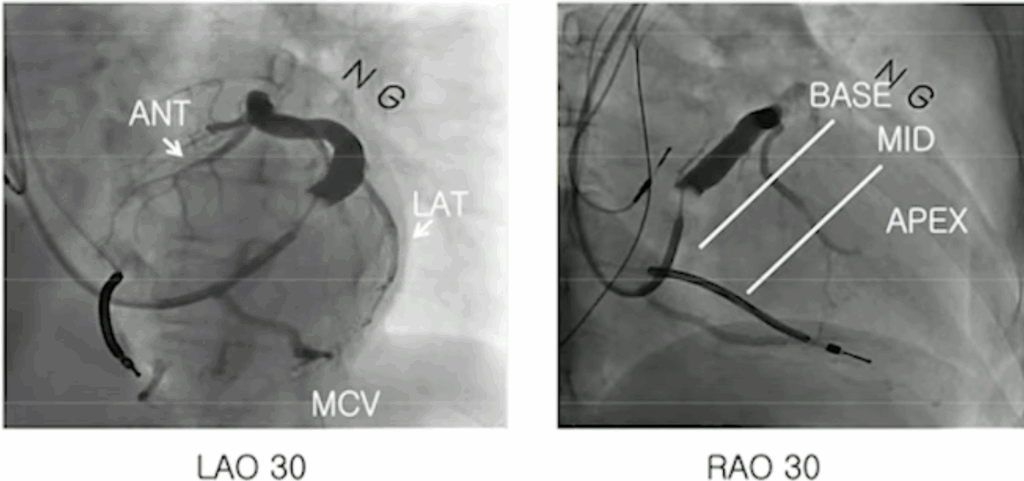
In the LAO view, you visualize the two “discs” of the right ventricle, with the right-sided structures on the left of the screen and the left-sided structures on the right.
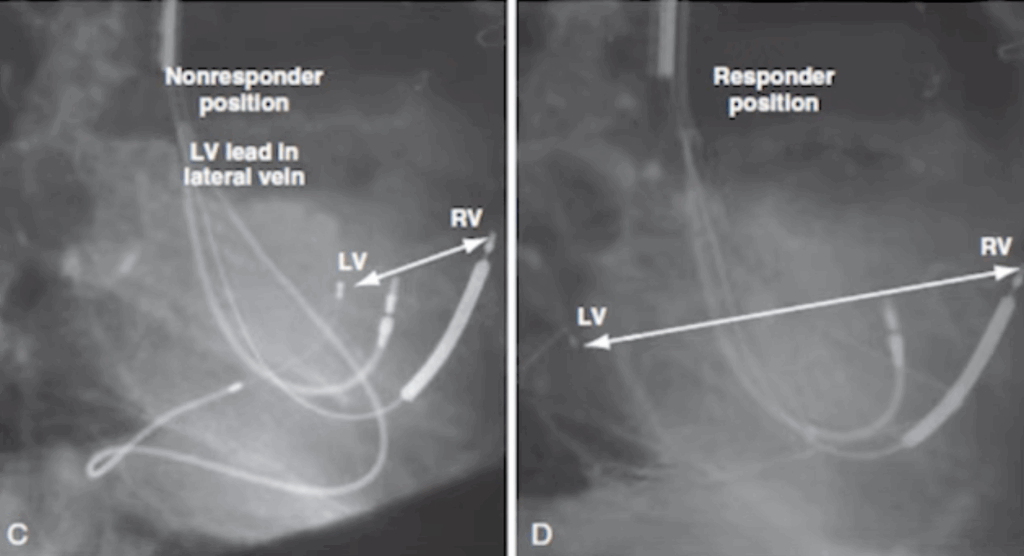
For LV pacing, the goal is to place the LV lead as far as possible from the RV lead to achieve optimal ventricular synchrony.
This is also the reason why the RV lead is placed first: once its position is fixed, you can determine exactly where the LV lead should be positioned to maximize separation and improve resynchronization.
The LAO view is essential, because it allows you to assess whether your chosen LV pacing site is likely to deliver good long-term CRT response.
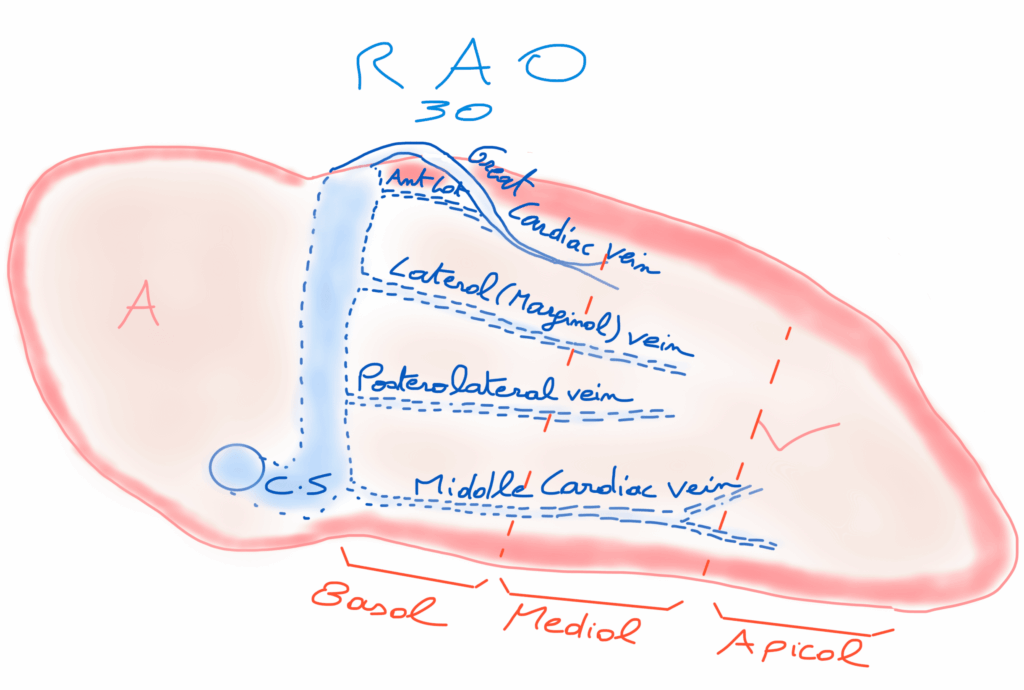
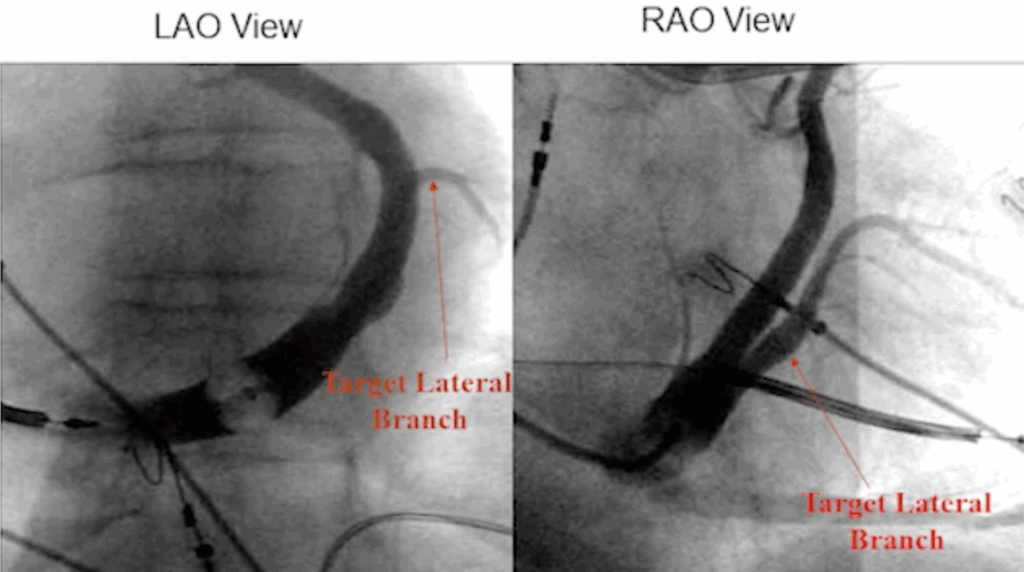
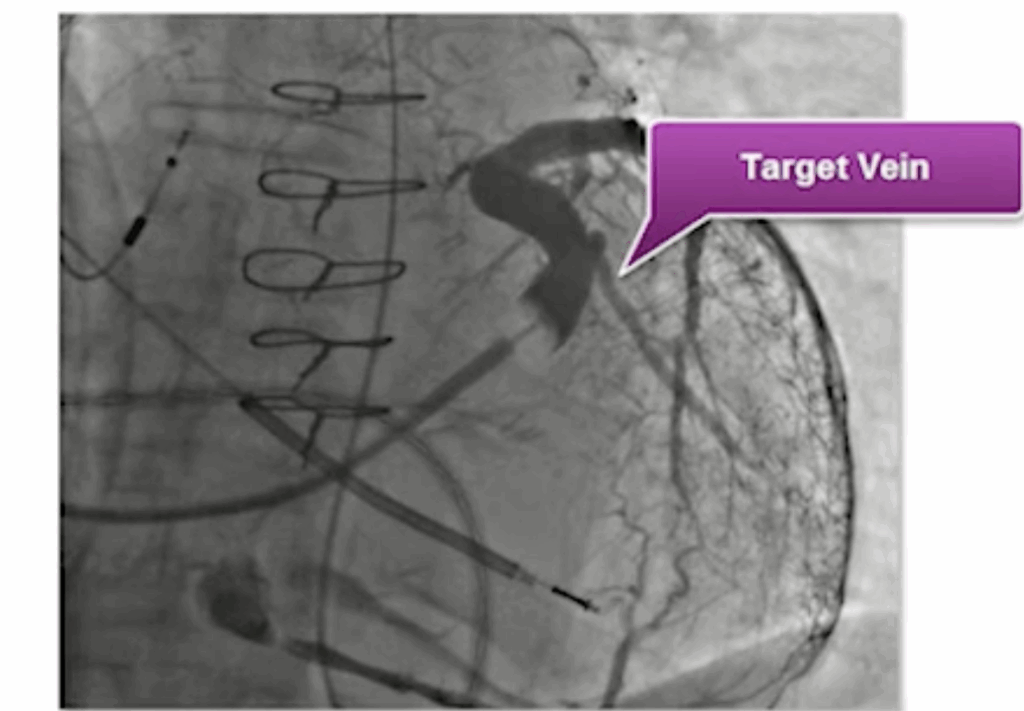
Practically, you target lateral venous branches located between 2 and 5 o’clock, ideally the posterolateral or lateral veins, which usually provide the most favorable electrical and mechanical delay.