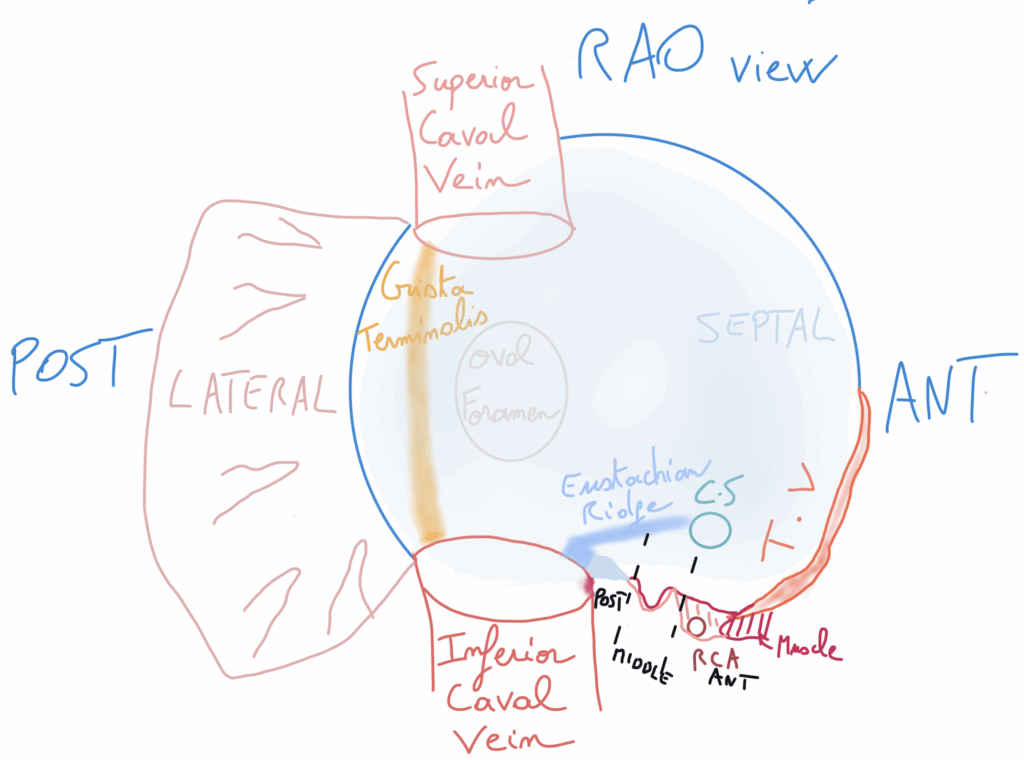
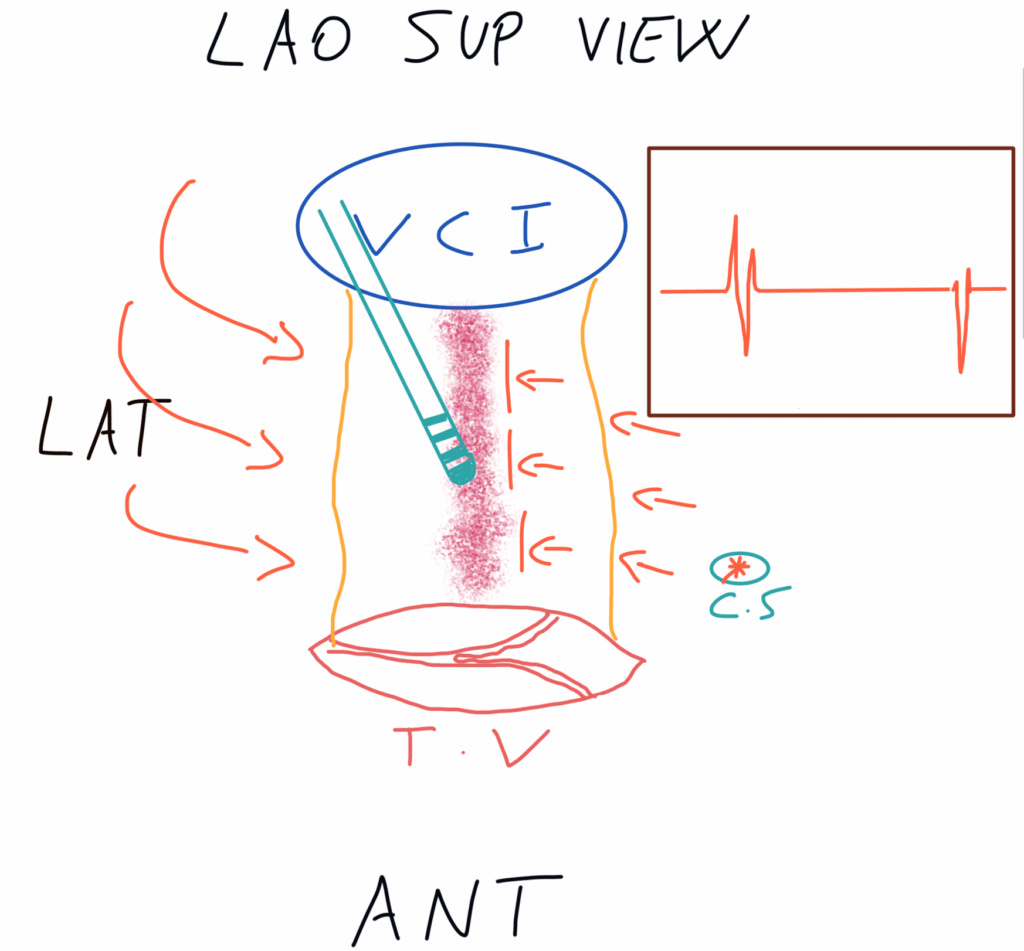
Here you have an RAO view. In front of us, we are looking at the septal aspect of the right atrium. On the right side, you can see the tricuspid valve with the right ventricle superior to it, and inferiorly the superior and inferior vena cava, respectively.
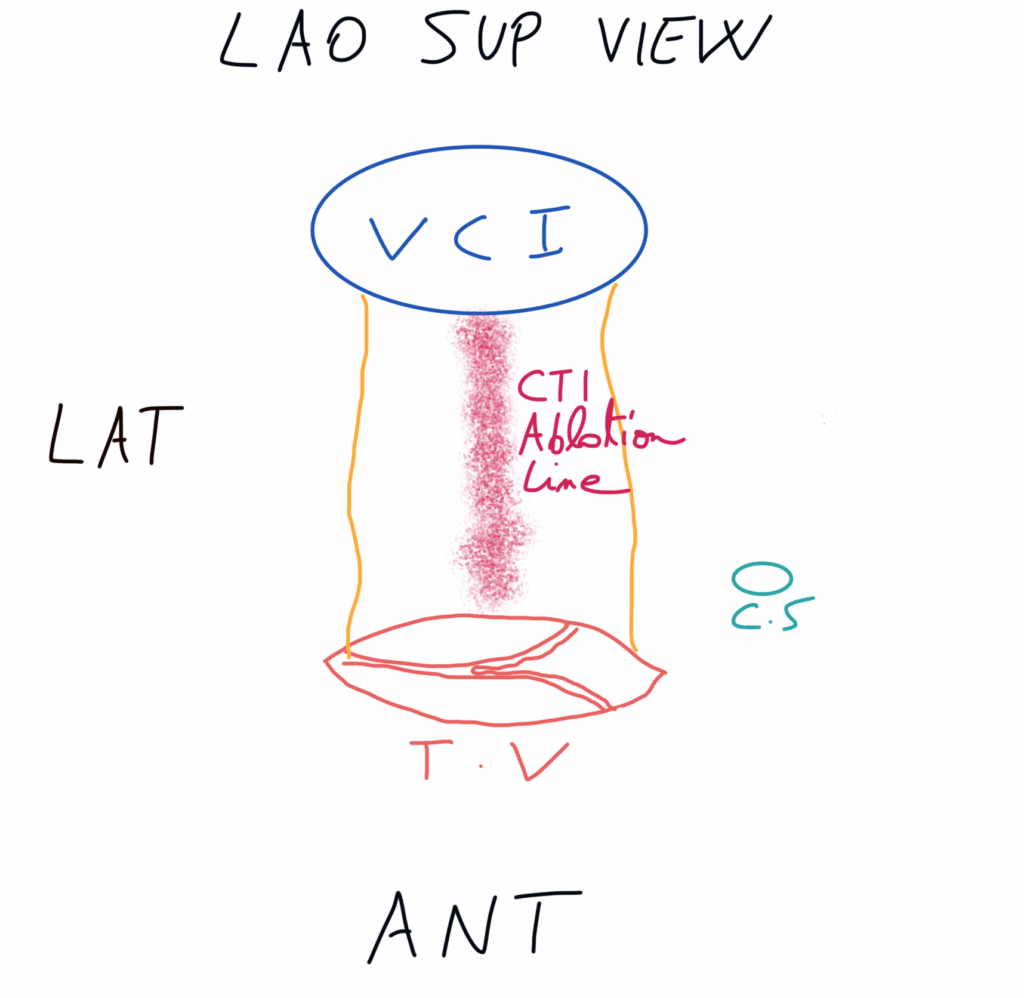
The area of interest is the CTI, which in the RAO view lies between the tricuspid valve and the inferior vena cava.
In the RAO view, the CTI is divided from front to back into anterior, middle, and posterior portions. It originates at the tricuspid valve and can extend toward the inferior vena cava.