LBBAP
Introduction
Right ventricular pacing is a bit like trying to choreograph a dance routine where one dancer jumps in too early, leaving the other hopelessly behind—talk about awkward timing! When the septum gets excited too soon and the left ventricular free wall lags behind, the heart ends up with messy electrical signals and clumsy contractions. Clinically speaking, this disco disaster can lead to pacing-induced cardiomyopathy in nearly 20% of patients, and unfortunately, increases the risk of heart failure-related hospital visits down the road (1)
The idea of conduction system pacing isn’t exactly breaking news—think of it as a vintage classic! More than 50 years ago, Scherlag and colleagues already showed us how to briefly catch the beat of the His bundle. However, it took another three decades for Deshmukh and friends to prove we could keep the rhythm going permanently. Good things come to those who wait (2)
Anatomy of the Cardiac Conduction System
How to Implant His Bundle and Left Bundle Pacing Leads: Tips and Pearls. Shunmuga Sundaram Ponnusamy, Pugazhendhi Vijayaraman. Card Fail Rev . 2021 Aug 6:7:e13. doi: 10.15420/cfr.2021.04. eCollection 2021 Mar.
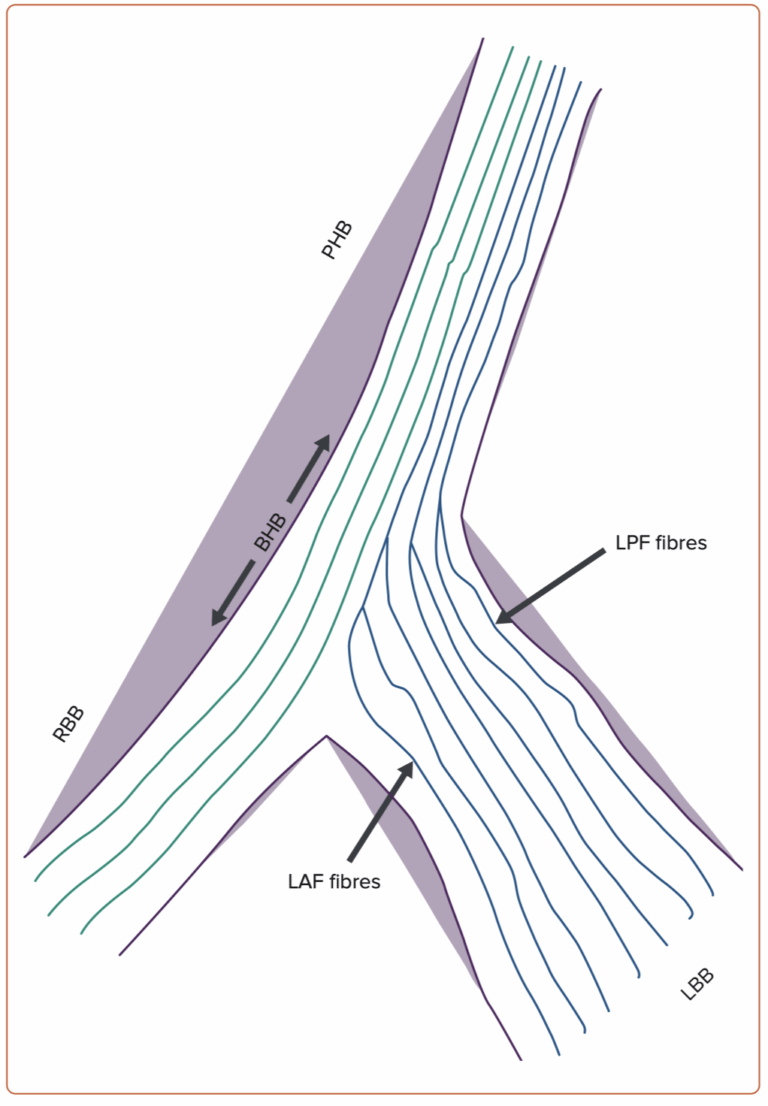
Imagine the His bundle as a highway that splits into two main roads: one heading left (the left bundle branch, LBB) and one continuing straight to the right (the right bundle branch, RBB). Now, the cool part is this highway actually has two segments: first, the ‘penetrating’ part (PHB) dives into the heart muscle, and then the ‘branching’ part (BHB) prepares the lanes to split. Interestingly, even from the start, fibers already know whether they’re destined to take the exit left or keep cruising straight ahead—talk about having a built-in GPS!
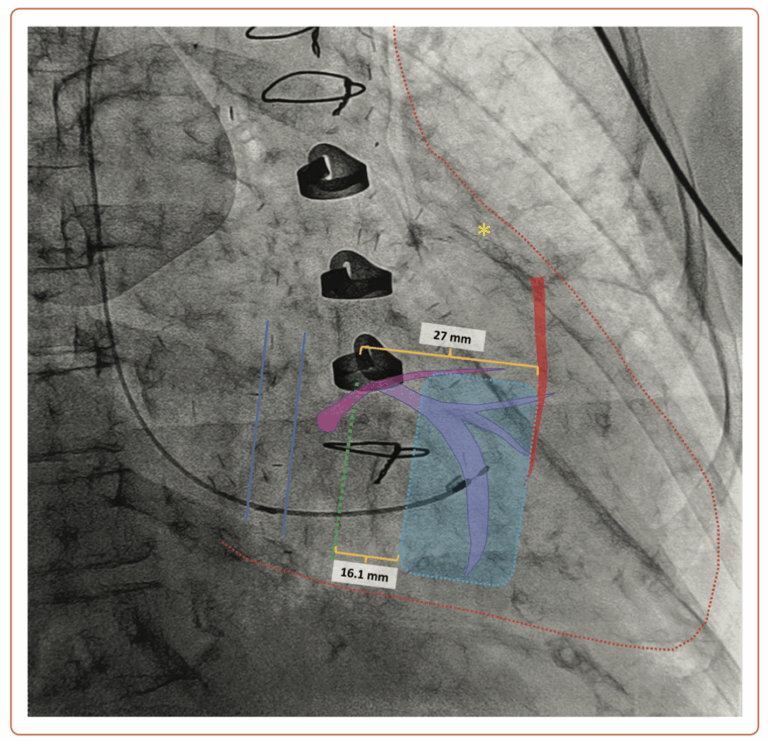
Think of the heart as a tricky neighborhood: the coronary sinus (between the blue lines) is like a clear alleyway, while the tricuspid valve (green dashed line) sits just slightly next door. In this patient, we’ve spotted the left anterior descending artery (marked by the yellow star) with its first septal perforator (highlighted in red) branching off about 27 mm away from the tricuspid valve’s doorstep. To keep things friendly and not make the valve leak worse, the pacing lead needs its own ‘personal space’—at least 16 mm away. That means the ideal spot (the safe zone, marked by the dashed blue area) for placing the lead is comfortably between 16 and 27 mm from the valve. No awkward neighbors here!
LBB capture
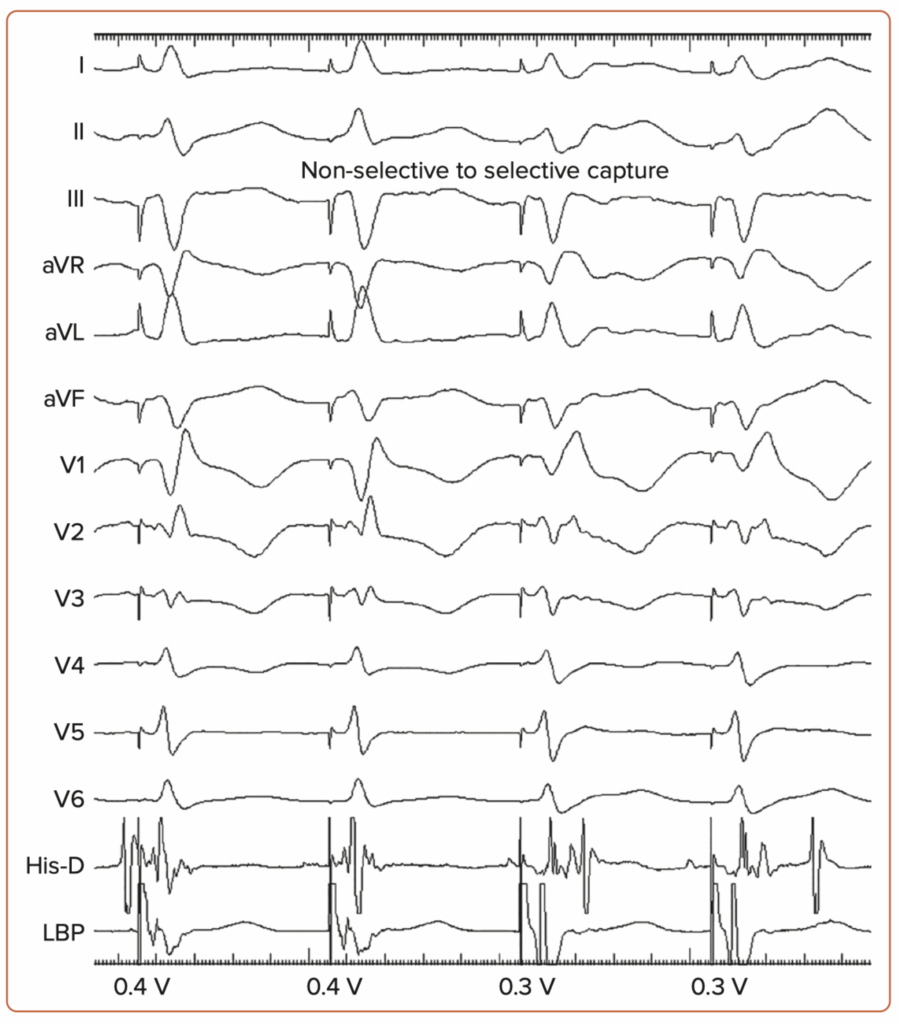
LBB capture is confirmed by paced QRS morphology of RBB delay pattern (qR or rSR in lead V1) along with any one of the following criteria: (3,4)
- Demonstration of non-selective to selective capture or non-selective to septal capture transition during threshold testing.
- Abrupt shortening of R-wave peak times (RWPT), as measured in leads V5 or V6 during lead implantation at the mid-septum and subsequent short and constant RWPT at the final site.
- Demonstration of LBB potential.
- Programmed deep septal stimulation from the pacing lead to demonstrate conduction system capture, especially selective capture.
- Meeting physiology-based electrocardiographic criteria, namely paced RWPT in V6 (measured from QRS onset) equals the native RWPT and paced RWPT (measured from the stimulus) equals the LBBP potential to V6.
Technique
Fluoroscopy view at RAO 30°: Imagine finding the perfect spot on the septum as gently steering a ship—with just a slight counterclockwise twist—to hit that sweet spot! You’re looking for a classic ‘W’-shaped pattern on lead V1, with a little notch right at the bottom of the wave, a nice tall R wave on lead II, an RS pattern on lead III, and opposite waveforms on leads aVR and aVL. But don’t worry if you don’t always see the famous ‘W’—it likes to play hide-and-seek and disappears about 20% of the time. Once you’ve found your spot, hold your sheath steady, pointing its hub towards your right hand (like aiming between 3 and 4 o’clock), so it’s perfectly perpendicular to the septum.
After you’ve nailed the spot, you’ve got two cool ways to deploy your lead: (5)
The classic method: slowly and steadily, keeping an eye on the paced QRS shape and impedance;
The PVC-guided turbo mode: fast deployment, using those spontaneous extra beats (PVCs) as your personal GPS!
How to Implant His Bundle and Left Bundle Pacing Leads: Tips and Pearls. Shunmuga Sundaram Ponnusamy, Pugazhendhi Vijayaraman. Card Fail Rev . 2021 Aug 6:7:e13. doi: 10.15420/cfr.2021.04. eCollection 2021 Mar.
Conventional Technique:
Deploying the pacing lead here is a bit like slowly turning a screw—careful and steady wins the race! You’ll make gentle rotations, always checking three key clues to confirm you’re on track:
Paced QRS shape: Watch that notch in lead V1 climb upwards into a neat little R wave.
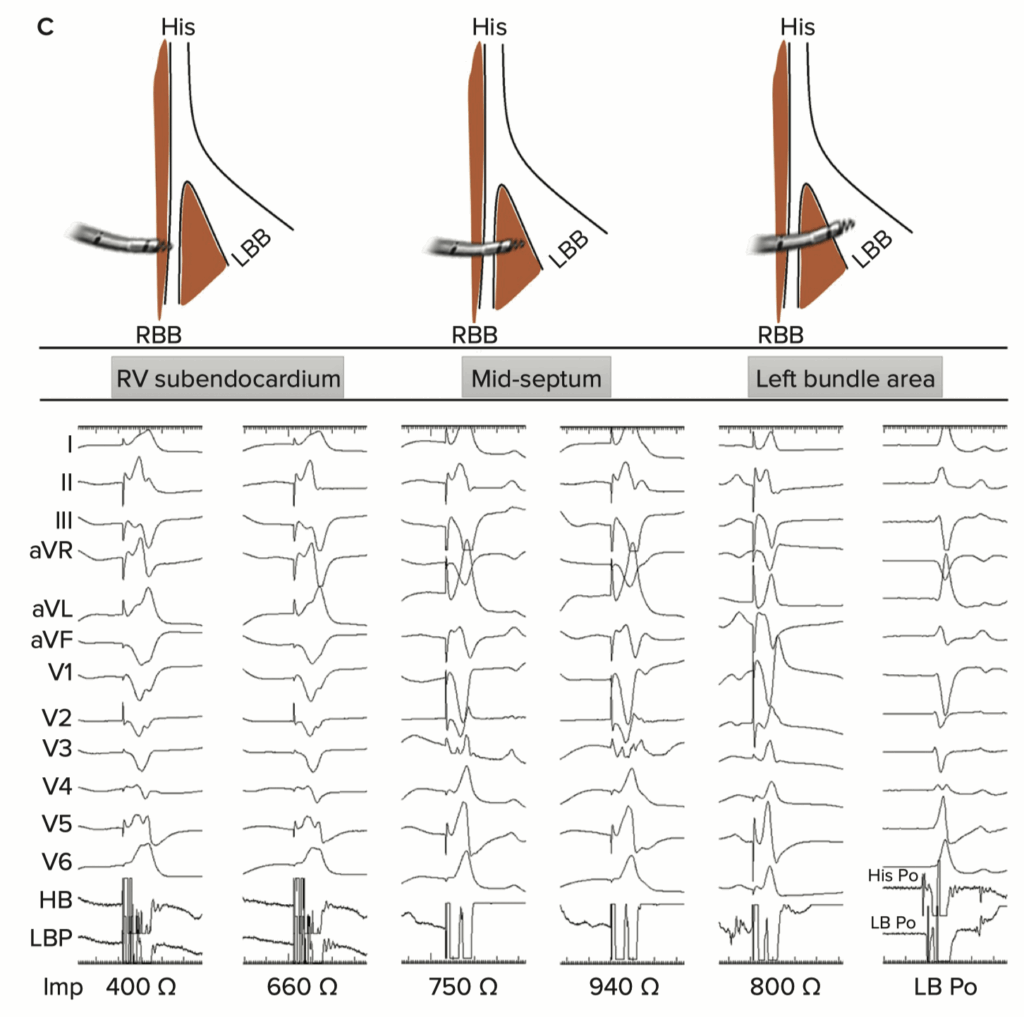
Unipolar pacing impedance: You’ll see impedance steadily rise until it suddenly drops by about 100–200 Ω when you reach the sweet spot (the LV subendocardium).
Myocardial COI signals on the lead electrogram (think of this as your heart’s own ‘green light’).
But beware—if impedance suddenly plunges more than 200 Ω, drops below 400 Ω, or you lose that nice R wave amplitude with the disappearance of COI, you’ve probably gone a bit too far (oops!), and the lead might have poked through into the LV cavity.
How to Implant His Bundle and Left Bundle Pacing Leads: Tips and Pearls. Shunmuga Sundaram Ponnusamy, Pugazhendhi Vijayaraman. Card Fail Rev . 2021 Aug 6:7:e13. doi: 10.15420/cfr.2021.04. eCollection 2021 Mar.
“Turbo” Technique:
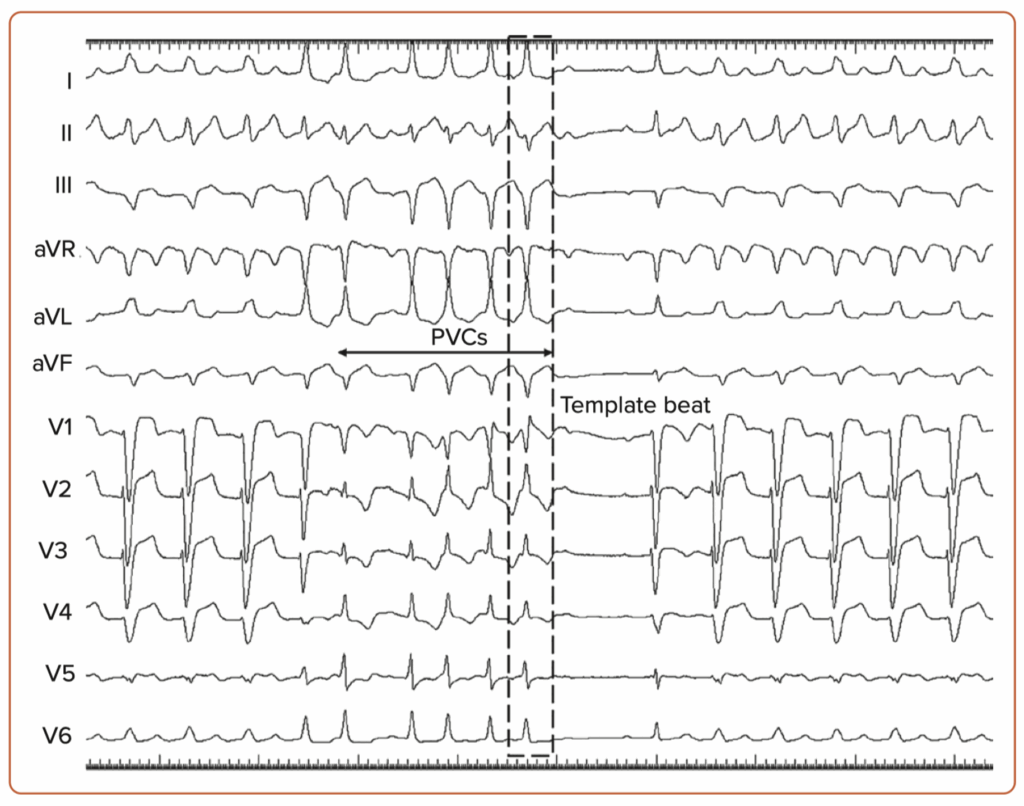
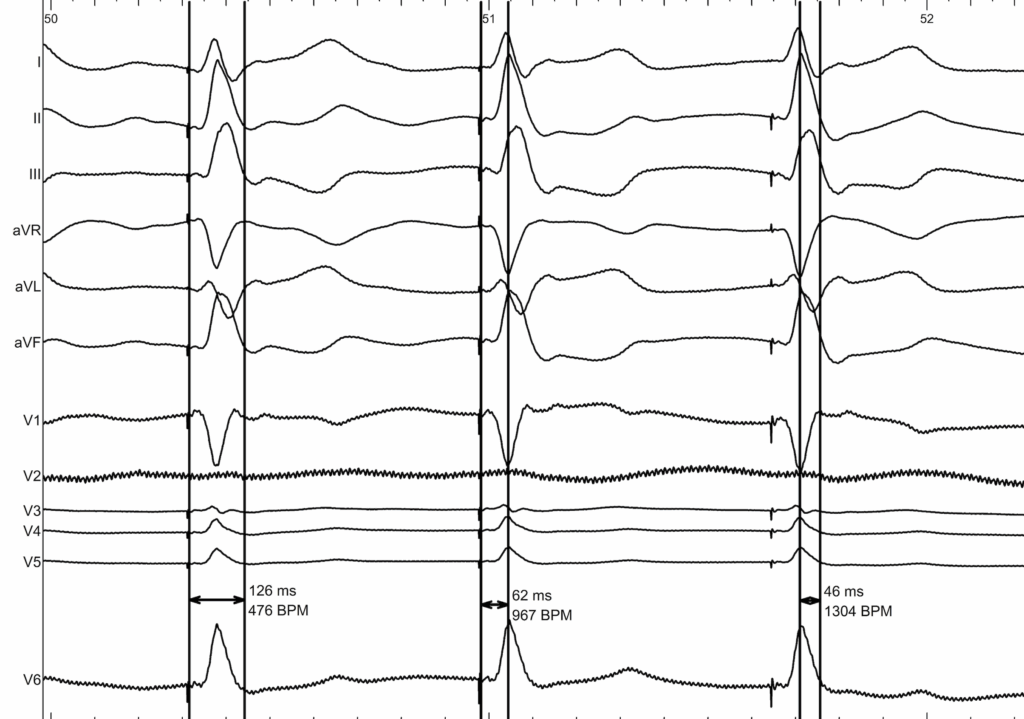
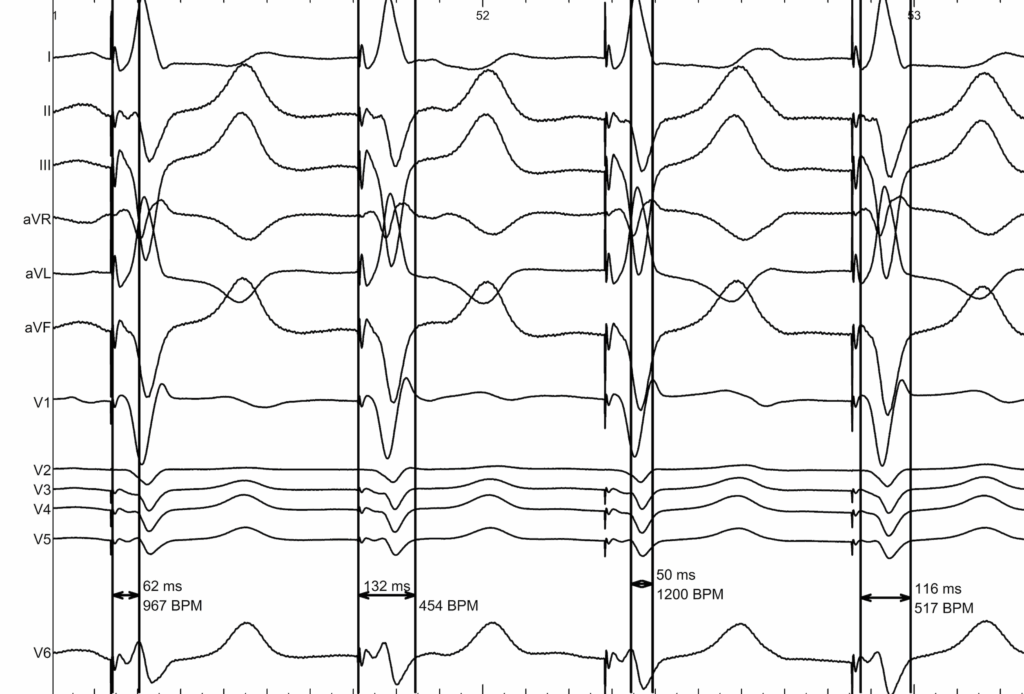
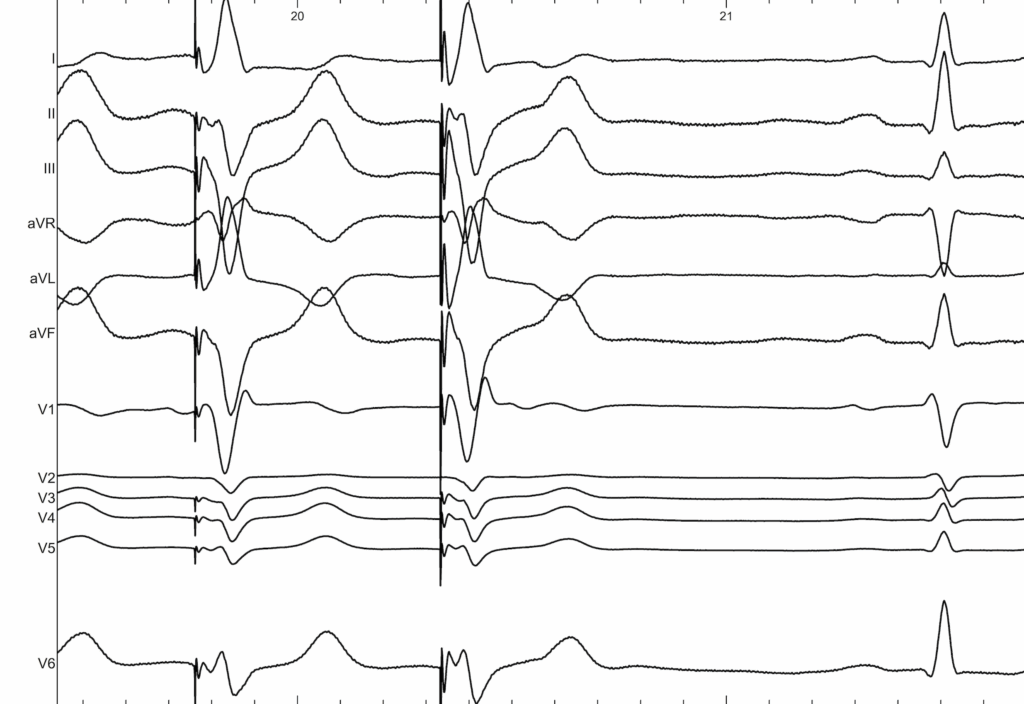
With this method, you crank the lead in quickly (imagine rapid-fire twists), and you’ll often spot some bonus beats (PVCs) as your lead digs into the septum. In the LAO 30° view, you’ll see your lead making progress clearly. Keep an eye on those PVC waveforms—initially wide and messy (QS pattern) in lead V1, gradually becoming narrow and tidy (with right bundle branch delay: qR/rSR). You’re “aha!” moment comes when a clean, narrow PVC (less than 130 ms)—your perfect template—appears. Stop twisting right there! You’ve hit the jackpot. This method is super handy because it saves fluoroscopy time, reduces heart muscle injury, and helps avoid accidentally poking all the way through the septum
Time for some rapid action! Quickly spin the lead into the septum while observing from the LAO 30° view—think of it as fast-forwarding through a movie. As the lead dives in, you’ll spot PVCs (those spontaneous bonus beats) popping up. Initially, these PVCs look wide and messy (QS pattern in V1), but they’ll sharpen up into neat, narrow beats (qR/rSR pattern) as you cross from right to left. Your ‘Template beat’—a nice narrow PVC under 130 ms—is your sign to immediately hit pause. Congrats, you’ve found the ideal spot! This handy trick reduces X-ray exposure, minimizes injury to the heart muscle, and keeps you from accidentally poking too far.
Once you’re there, you can pace at 10 V and carefully add a few more twists to achieve the shortest RWPT (usually under 90 ms, though it might sometimes stretch longer if the patient has heart muscle thickening or conduction issues).
After confirming you’re in the right spot (LBB capture), gently slide the sheath back into the right atrium, making sure your lead has just enough slack. You might notice an ‘alpha loop’ forming—that pesky loop can be straightened out easily in the RAO view with a gentle backward pull and a slight counterclockwise twist. Don’t forget a final check of your pacing settings in both unipolar and bipolar modes.
Pro tip: Keep your gloves and lead dry during rapid rotations to avoid slipping! And if your basal septum isn’t playing nice due to scarring, aim your lead a bit lower and further back—right at the left posterior fascicle in the mid-septal region.
How to Implant His Bundle and Left Bundle Pacing Leads: Tips and Pearls. Shunmuga Sundaram Ponnusamy, Pugazhendhi Vijayaraman. Card Fail Rev . 2021 Aug 6:7:e13. doi: 10.15420/cfr.2021.04. eCollection 2021 Mar.
Example of Left Bundle Branch Area Pacing
REFERENCES :
1 – Kurshid S, Epstein AE, Verdino RJ, et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm 2014;11:1619–25. https://doi. org/10.1016/j.hrthm.2014.05.040; PMID: 24893122.
2 -Deshmukh P, Casavant DA, Romanyshyn M, et al. Permanent, direct His-bundle pacing: a novel approach to cardiac pacing in patients with normal His–Purkinje activation. Circulation 2000;101:869–77. https://doi. org/10.1161/01.CIR.101.8.869; PMID: 10694526.
3 – Ponnusamy SS, Arora V, Namboodiri N, et al. Left bundle branch pacing: a comprehensive review. J Cardiovasc Electrophysiol 2020;31:2462–73 https://doi.org/10.1111/ jce.14681; PMID: 32681681.
4 – Jastrzebski M, Keilbasa G, Curila K, et al. Physiology-based electrocardiographic criteria for left bundle branch capture. Heart Rhythm 2021;18:935–43. https://doi. org/10.1016/j.hrthm.2021.02.021; PMID: 33677102.
5 – Ponnusamy SS, Ganesan V, Syed T, et al. Template beat: a novel marker for left bundle branch capture during physiological pacing. Circ Arrhythm Electrophysiol
6 – How to Implant His Bundle and Left Bundle Pacing Leads: Tips and Pearls. Shunmuga Sundaram Ponnusamy, Pugazhendhi Vijayaraman. Card Fail Rev . 2021 Aug 6:7:e13. doi: 10.15420/cfr.2021.04. eCollection 2021 Mar.